

Improved efficacy of mitoxantrone in patients with castration-resistant prostate cancer after vaccination with GM-CSF-transduced allogeneic prostate cancer cells
- PMID: 27141390
- PMCID: PMC4839338
- DOI: 10.1080/2162402X.2015.1105431
Improved efficacy of mitoxantrone in patients with castration-resistant prostate cancer after vaccination with GM-CSF-transduced allogeneic prostate cancer cells
Abstract
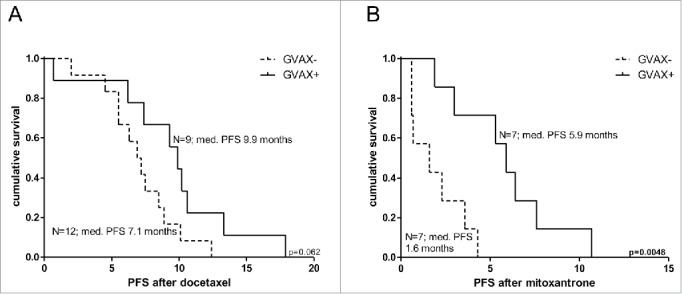
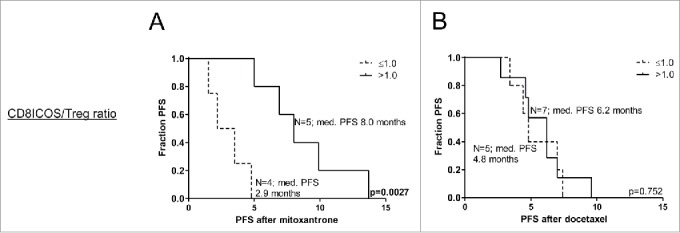
Previous vaccination studies in patients with castration-resistant prostate cancer (CRPC) showed improved survival without prolongation of progression-free survival (PFS). This might be explained by enhanced efficacy of subsequent therapies because of heightened immune status. We therefore evaluated the efficacy of chemotherapy in CRPC patients after immunotherapy. We retrospectively analyzed 28 patients who were treated with ipilimumab and GVAX, an allogeneic vaccine, and 21 patients who were randomized to GVAX or no vaccination. To study whether immune status was related to the efficacy of chemotherapy, frequencies of myeloid and lymphocyte subsets were determined. Of 28 patients treated with GVAX and ipilimumab, 23 patients received docetaxel and 13 patients mitoxantrone. Median PFS after docetaxel was 6.4 mo (range 0.8-11.2), while median PFS after mitoxantrone was markedly longer than expected (4.8 mo; range 1.4-13.7). High CD8+ICOS+ Tcell/Treg and pDC/mMDSC ratios were associated with relatively long PFS after mitoxantrone, suggesting a correlation between activated immune status and benefit of mitoxantrone. Analysis of 21 patients, randomized to GVAX or not, revealed a median PFS after docetaxel of 9.9 mo for vaccinated patients and 7.1 mo for unvaccinated patients. Interestingly, PFS after mitoxantrone (n = 14) was significantly longer in vaccinated patients as compared to controls (5.9 vs. 1.6 mo, p = 0.0048). In conclusion, mitoxantrone seems more effective in CRPC patients after immunotherapy, which may be related to the immune-stimulating effect of mitoxantrone in patients with heightened antitumor immunity. As this was a retrospective study with limited sample size, prospective studies are warranted to definitively show proof of principle.
Keywords: Cancer vaccines; GVAX; chemotherapy; docetaxel; immunotherapy; mitoxantrone; prostate cancer.
Figures
Similar articles
-
Myeloid derived suppressor and dendritic cell subsets are related to clinical outcome in prostate cancer patients treated with prostate GVAX and ipilimumab.J Immunother Cancer. 2014 Sep 16;2:31. doi: 10.1186/s40425-014-0031-3. eCollection 2014. J Immunother Cancer. 2014. PMID: 26196012 Free PMC article.
-
Combined immunotherapy with granulocyte-macrophage colony-stimulating factor-transduced allogeneic prostate cancer cells and ipilimumab in patients with metastatic castration-resistant prostate cancer: a phase 1 dose-escalation trial.Lancet Oncol. 2012 May;13(5):509-17. doi: 10.1016/S1470-2045(12)70007-4. Epub 2012 Feb 10. Lancet Oncol. 2012. PMID: 22326922
-
The evolving role of immunotherapy in prostate cancer.Ann Oncol. 2012 Sep;23 Suppl 8:viii22-7. doi: 10.1093/annonc/mds259. Ann Oncol. 2012. PMID: 22918924 Review.
-
The influence of prior abiraterone treatment on the clinical activity of docetaxel in men with metastatic castration-resistant prostate cancer.Eur Urol. 2014 Oct;66(4):646-52. doi: 10.1016/j.eururo.2014.01.018. Epub 2014 Jan 24. Eur Urol. 2014. PMID: 24491307 Free PMC article.
-
Current vaccination strategies for prostate cancer.Eur Urol. 2012 Feb;61(2):290-306. doi: 10.1016/j.eururo.2011.09.020. Epub 2011 Oct 3. Eur Urol. 2012. PMID: 22001436 Review.
Cited by
-
Pancreatic Cancer and Immunotherapy: A Clinical Overview.Cancers (Basel). 2021 Aug 17;13(16):4138. doi: 10.3390/cancers13164138. Cancers (Basel). 2021. PMID: 34439292 Free PMC article. Review.
-
Vaccine-Linked Chemotherapy Approach: Additive Effects of Combining the Listeria monocytogenes-Based Vaccine Lm3Dx_NcSAG1 With the Bumped Kinase Inhibitor BKI-1748 Against Neospora caninum Infection in Mice.Front Vet Sci. 2022 Jun 27;9:901056. doi: 10.3389/fvets.2022.901056. eCollection 2022. Front Vet Sci. 2022. PMID: 35832325 Free PMC article.
-
Trial Watch: Immunostimulatory monoclonal antibodies for oncological indications.Oncoimmunology. 2017 Aug 30;6(12):e1371896. doi: 10.1080/2162402X.2017.1371896. eCollection 2017. Oncoimmunology. 2017. PMID: 29209572 Free PMC article. Review.
-
Trial Watch: Oncolytic viro-immunotherapy of hematologic and solid tumors.Oncoimmunology. 2018 Aug 27;7(12):e1503032. doi: 10.1080/2162402X.2018.1503032. eCollection 2018. Oncoimmunology. 2018. PMID: 30524901 Free PMC article. Review.
-
Rational Design, Synthesis and Binding Affinity Studies of Anthraquinone Derivatives Conjugated to Gonadotropin-Releasing Hormone (GnRH) Analogues towards Selective Immunosuppression of Hormone-Dependent Cancer.Int J Mol Sci. 2023 Oct 16;24(20):15232. doi: 10.3390/ijms242015232. Int J Mol Sci. 2023. PMID: 37894912 Free PMC article.
References
-
- Neppl-Huber C, Zappa M, Coebergh JW, Rapiti E, Rachtan J, Holleczek B, Rosso S, Aareleid T, Brenner H, Gondos A. Changes in incidence, survival and mortality of prostate cancer in Europe and the United States in the PSA era: additional diagnoses and avoided deaths. Ann Oncol 2012; 23:1325-34; PMID:21965474; http://dx.doi.org/10.1093/annonc/mdr414 - DOI - PubMed
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65:87-108; PMID:25651787; http://dx.doi.org/10.3322/caac.21262 - DOI - PubMed
-
- Debes JD, Tindall DJ. Mechanisms of androgen-refractory prostate cancer. N Engl J Med 2004; 351:1488-90; PMID:15470210; http://dx.doi.org/10.1056/NEJMp048178 - DOI - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, Lara PN Jr, Jones JA, Taplin ME, Burch PA, Berry D, Moinpour C, Kohli M et al.. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med 2004; 351:1513-20; PMID:15470214; http://dx.doi.org/10.1056/NEJMoa041318 - DOI - PubMed
-
- Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Théodore C, James ND, Turesson I et al.. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004; 351:1502-12; PMID:15470213; http://dx.doi.org/10.1056/NEJMoa040720 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials