

Addition of dipeptidyl peptidase-4 inhibitors to sulphonylureas and risk of hypoglycaemia: systematic review and meta-analysis
- PMID: 27142267
- PMCID: PMC4854021
- DOI: 10.1136/bmj.i2231
Addition of dipeptidyl peptidase-4 inhibitors to sulphonylureas and risk of hypoglycaemia: systematic review and meta-analysis
Abstract
Objective: To quantify the risk of hypoglycaemia associated with the concomitant use of dipeptidyl peptidase-4 (DPP-4) inhibitors and sulphonylureas compared with placebo and sulphonylureas.
Design: Systematic review and meta-analysis.
Data sources: Medline, ISI Web of Science, SCOPUS, Cochrane Central Register of Controlled Trials, and clinicaltrial.gov were searched without any language restriction.
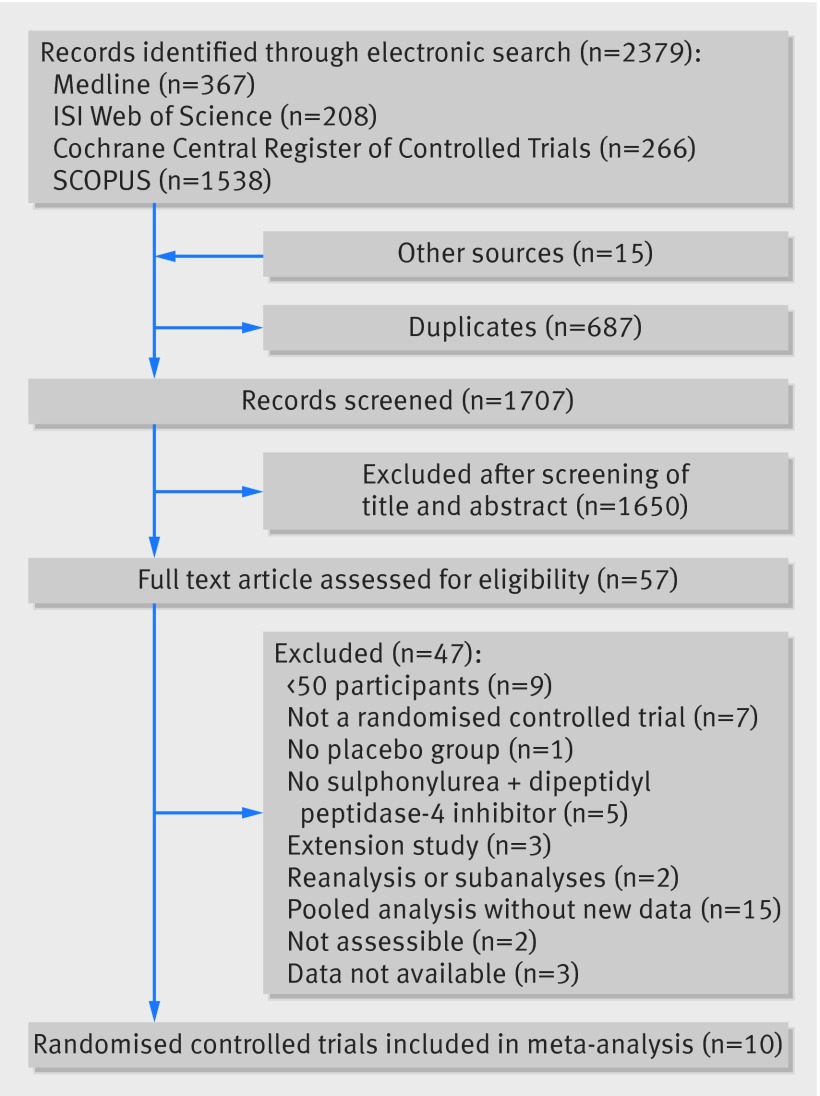
Study selection: Placebo controlled randomised trials comprising at least 50 participants with type 2 diabetes treated with DPP-4 inhibitors and sulphonylureas.
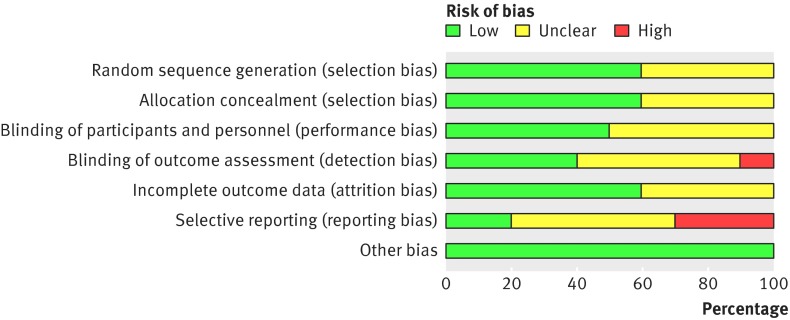
Review methods: Risk of bias in each trial was assessed using the Cochrane Collaboration tool. The risk ratio of hypoglycaemia with 95% confidence intervals was computed for each study and then pooled using fixed effect models (Mantel Haenszel method) or random effect models, when appropriate. Subgroup analyses were also performed (eg, dose of DPP-4 inhibitors). The number needed to harm (NNH) was estimated according to treatment duration.
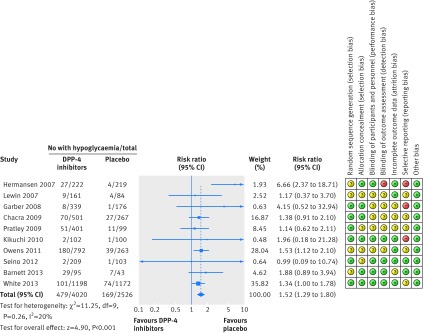
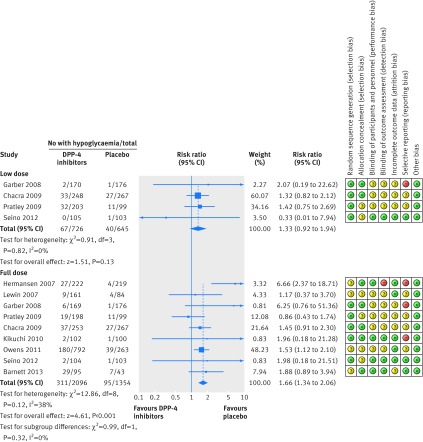
Results: 10 studies were included, representing a total of 6546 participants (4020 received DPP-4 inhibitors plus sulphonylureas, 2526 placebo plus sulphonylureas). The risk ratio of hypoglycaemia was 1.52 (95% confidence interval 1.29 to 1.80). The NNH was 17 (95% confidence interval 11 to 30) for a treatment duration of six months or less, 15 (9 to 26) for 6.1 to 12 months, and 8 (5 to 15) for more than one year. In subgroup analysis, no difference was found between full and low doses of DPP-4 inhibitors: the risk ratio related to full dose DPP-4 inhibitors was 1.66 (1.34 to 2.06), whereas the increased risk ratio related to low dose DPP-4 inhibitors did not reach statistical significance (1.33, 0.92 to 1.94).
Conclusions: Addition of DPP-4 inhibitors to sulphonylurea to treat people with type 2 diabetes is associated with a 50% increased risk of hypoglycaemia and to one excess case of hypoglycaemia for every 17 patients in the first six months of treatment. This highlights the need to respect recommendations for a decrease in sulphonylureas dose when initiating DPP-4 inhibitors and to assess the effectiveness of this risk minimisation strategy.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Diabetes: Hypoglycaemia risk with dual use of DPP-4 inhibitors and sulphonylureas.Nat Rev Endocrinol. 2016 Jul;12(7):374. doi: 10.1038/nrendo.2016.80. Epub 2016 May 20. Nat Rev Endocrinol. 2016. PMID: 27199288 No abstract available.
-
Review: In type 2 diabetes, adding dipeptidyl peptidase-4 inhibitors to sulphonylureas increases hypoglycemia.Ann Intern Med. 2016 Aug 16;165(4):JC20. doi: 10.7326/ACPJC-2016-165-4-020. Ann Intern Med. 2016. PMID: 27538181 No abstract available.
References
-
- Kilbridge PM, Campbell UC, Cozart HB, Mojarrad MG. Automated surveillance for adverse drug events at a community hospital and an academic medical center. J Am Med Inform Assoc 2006;13:372-7. 10.1197/jamia.M2069 pmid:16622159. - DOI - PMC - PubMed
-
- Goto A, Arah OA, Goto M, Terauchi Y, Noda M. Severe hypoglycaemia and cardiovascular disease: systematic review and meta-analysis with bias analysis. BMJ 2013;347:f4533 10.1136/bmj.f4533 pmid:23900314. - DOI - PubMed
-
- Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 2010;375:481-9. 10.1016/S0140-6736(09)61969-3 pmid:20110121. - DOI - PubMed
-
- Bonds DE, Miller ME, Bergenstal RM, et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ 2010;340:b4909 10.1136/bmj.b4909 pmid:20061358. - DOI - PMC - PubMed
-
- Gerstein HC, Miller ME, Genuth S, et al. ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med 2011;364:818-28. 10.1056/NEJMoa1006524 pmid:21366473. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous