

2016 AAFP Guidelines for the Management of Feline Hyperthyroidism
- PMID: 27143042
- PMCID: PMC11132203
- DOI: 10.1177/1098612X16643252
2016 AAFP Guidelines for the Management of Feline Hyperthyroidism
Abstract
Clinical context: Since 1979 and 1980 when the first reports of clinical feline hyperthyroidism (FHT) appeared in the literature, our understanding of the disease has evolved tremendously. Initially, FHT was a disease that only referral clinicians treated. Now it is a disease that primary clinicians routinely manage. Inclusion of the measurement of total thyroxine concentration in senior wellness panels, as well as in diagnostic work-ups for sick cats, now enables diagnosis of the condition long before the cat becomes the classic scrawny, unkempt, agitated patient with a bulge in its neck. However, earlier recognition of the problem has given rise to several related questions: how to recognize the health significance of the early presentations of the disease; how early to treat the disease; whether to treat FHT when comorbid conditions are present; and how to manage comorbid conditions such as chronic kidney disease and cardiac disease with treatment of FHT. The 2016 AAFP Guidelines for the Management of Feline Hyperthyroidism (hereafter referred to as the Guidelines) will shed light on these questions for the general practitioner and suggest when referral may benefit the cat.
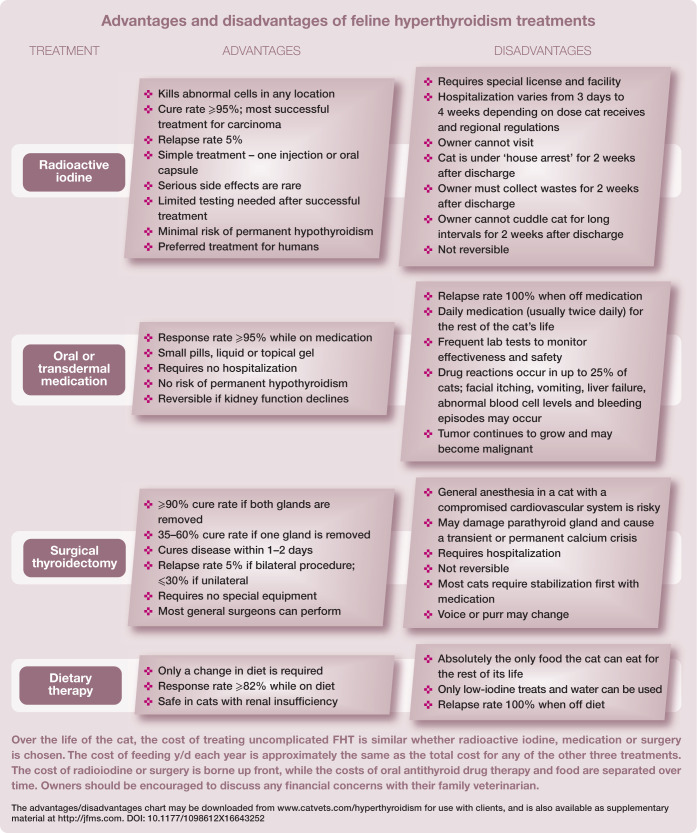
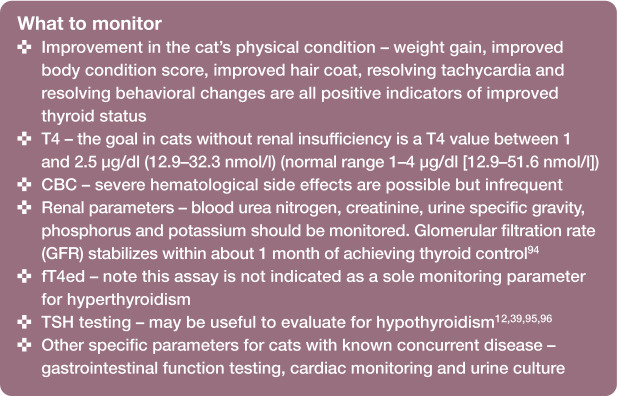
Scope: The Guidelines explain FHT as a primary disease process with compounding factors, and provide a concise explanation of what we know to be true about the etiology and pathogenesis of the disease.The Guidelines also:Distill the current research literature into simple recommendations for testing sequences that will avoid misdiagnosis and separate an FHT diagnosis into six clinical categories with associated management strategies.Emphasize the importance of treating all hyperthyroid cats, regardless of comorbidities, and outline the currently available treatments for the disease.Explain how to monitor the treated cat to help avoid exacerbating comorbid diseases.Dispel some of the myths surrounding certain aspects of FHT and replace them with an evidence-based narrative that veterinarians and their practice teams can apply to feline patients and communicate to their owners.
Evidence base: To help ensure better case outcomes, the Guidelines reflect currently available, evidenced-based knowledge. If research is lacking, or if a consensus does not exist, the expert panel of authors has made recommendations based on their extensive, cumulative clinical experience.
© The Author(s) 2016.
Conflict of interest statement
Duncan Ferguson, through a patent held by the University of Georgia, USA, has inventor rights over the molecular genetic sequence of feline TSH, and also gains some royalties from a monoclonal antibody against ovine/canine TSH that can be used in feline TSH immunoassays, but is not commercially available as such. The other AAFP Task Force members have no conflicts of interest to declare.
Figures

















References
-
- Peterson ME, Johnson JG, Andrews LK. Spontaneous hyperthyroidism in the cat. Proceedings of the American College of Veterinary Internal Medicine; Seattle, USA; 1979, p 108.
-
- Holzworth J, Theran P, Carpenter JL, et al.. Hyperthyroidism in the cat: ten cases. J Am Vet Med Assoc 1980; 176: 345–353. - PubMed
-
- Peterson ME. Feline hyperthyroidism: an animal model for toxic nodular goiter. J Endocrinol 2014; 223: T97–T114. - PubMed
-
- McLean JL, Lobetti RG, Schoeman JP. Worldwide prevalence and risk factors for feline hyperthyroidism: a review. J S Afr Vet Assoc 2014; 85: 1097. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
