

Assessing Barriers to Chronic Migraine Consultation, Diagnosis, and Treatment: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
- PMID: 27143127
- PMCID: PMC5084794
- DOI: 10.1111/head.12774
Assessing Barriers to Chronic Migraine Consultation, Diagnosis, and Treatment: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
Abstract
Objective: To assess the rates and predictors of traversing steps essential to good medical care for chronic migraine, including: (1) medical consultation, (2) accurate diagnosis, and (3) minimal pharmacologic treatment. Candidate predictors included socioeconomic, demographic, and headache-specific variables.
Background: Previous research has established that barriers to effective management for episodic migraine include the absence of health insurance, lack of appropriate medical consultation, failure to receive an accurate diagnosis, and not being offered a regimen with acute and preventive treatments.
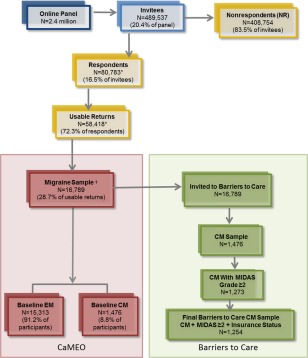
Methods/design: The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study, a longitudinal web-based panel study of migraine, included a cross-sectional module focused on patterns of and barriers to medical care. Participants eligible for this analysis met the study criteria for chronic migraine, had evidence of headache-related disability, and provided data on health insurance status. The main outcomes in the current analysis included the proportion of respondents who sought consultation for headache with a designated healthcare professional, self-reported receiving a diagnosis of chronic or transformed migraine, and received minimal pharmacologic treatment for headache with a focus on prescribed acute and preventive treatments.
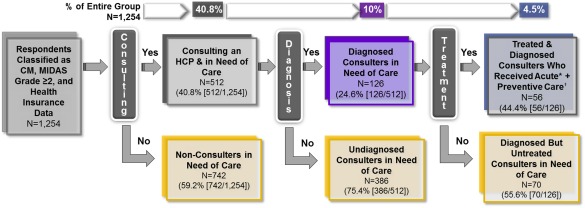
Results: In the CaMEO Study, 80,783 respondents provided study data, 16,789 (20.8% of respondents) met criteria for migraine, and 1476 (8.8% of those with migraine) met chronic migraine criteria. In total, 1254 participants (85.0% of those with chronic migraine) met inclusion criteria for this analysis. Of those, 512 respondents (40.8%) reported currently consulting with a healthcare professional for headache. Odds of consulting increased with increasing age (OR 1.02; 95% CI 1.01-1.03), body mass index (BMI) (OR 1.01; 95% CI 1.00-1.03), migraine-related disability (OR 1.02; 95% CI 1.00-1.04), and migraine severity (OR 1.16; 95% CI 1.11-1.22) and presence of health insurance (OR 4.61; 95% CI 3.05-6.96). Among those consulting a healthcare professional, 126 (24.6%) received an accurate diagnosis and 56 of those with a correct diagnosis (44.4%) received both acute and preventive pharmacologic treatments; odds of a CM diagnosis were higher for women (OR 1.93; 95% CI 1.03-3.61), those with greater migraine severity (OR 1.25; 95% CI 1.14-1.37), and those currently consulting a specialist (OR 2.38; 95% CI 1.54-3.69). No predictors of receiving appropriate treatment were identified among those currently consulting. Among our sample of people with chronic migraine, only 56 (4.5%) individuals successfully traversed the series of 3 barriers to successful chronic migraine care (ie, consulted a healthcare professional for migraine, received an accurate diagnosis, and were prescribed minimal acute and preventive pharmacologic treatments).
Conclusion: Our findings suggest that <5% of persons with chronic migraine traversed 3 barriers to receiving care for headache (consultation, diagnosis, and treatment), representing a large unmet need for improving care in this population. Predictors of consulting a healthcare professional included age, having health insurance, greater migraine-related disability, and greater migraine symptom severity. Among those consulting, predictors of an appropriate diagnosis included consulting a specialist, female sex, and greater migraine severity. Public health efforts are needed to improve outcomes for patients with chronic migraine by a range of interventions and educational efforts aimed at improving consultation rates, diagnostic accuracy, and adherence to minimal pharmacologic treatment.
Keywords: acute medication; barrier to care; chronic migraine; headache-related disability; migraine; preventive medication.
© 2016 The Authors Headache published by Wiley Periodicals, Inc. on behalf of American Headache Society.
Figures
References
-
- Headache Classification Committee of the International Headache Society . The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33:629‐808. - PubMed
-
- Goadsby PJ, Sprenger T. Current practice and future directions in the prevention and acute management of migraine. Lancet Neurol. 2010;9:285‐298. - PubMed
-
- Buse DC, Manack AN, Fanning KM, et al. Chronic migraine prevalence, disability, and sociodemographic factors: Results from the American Migraine Prevalence and Prevention Study. Headache. 2012;52:1456‐1470. - PubMed
-
- Wang SJ, Wang PJ, Fuh JL, Peng KP, Ng K. Comparisons of disability, quality of life, and resource use between chronic and episodic migraineurs: A clinic‐based study in Taiwan. Cephalalgia. 2013;33:171‐181. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
