

Usual blood pressure, atrial fibrillation and vascular risk: evidence from 4.3 million adults
- PMID: 27143136
- PMCID: PMC5407172
- DOI: 10.1093/ije/dyw053
Usual blood pressure, atrial fibrillation and vascular risk: evidence from 4.3 million adults
Abstract
Background: Although elevated blood pressure is associated with an increased risk of atrial fibrillation (AF), it is unclear if this association varies by individual characteristics. Furthermore, the associations between AF and a range of different vascular events are yet to be reliably quantified.
Methods: Using linked electronic health records, we examined the time to first diagnosis of AF and time to first diagnosis of nine vascular events in a cohort of 4.3 million adults, aged 30 to 90 years, in the UK.
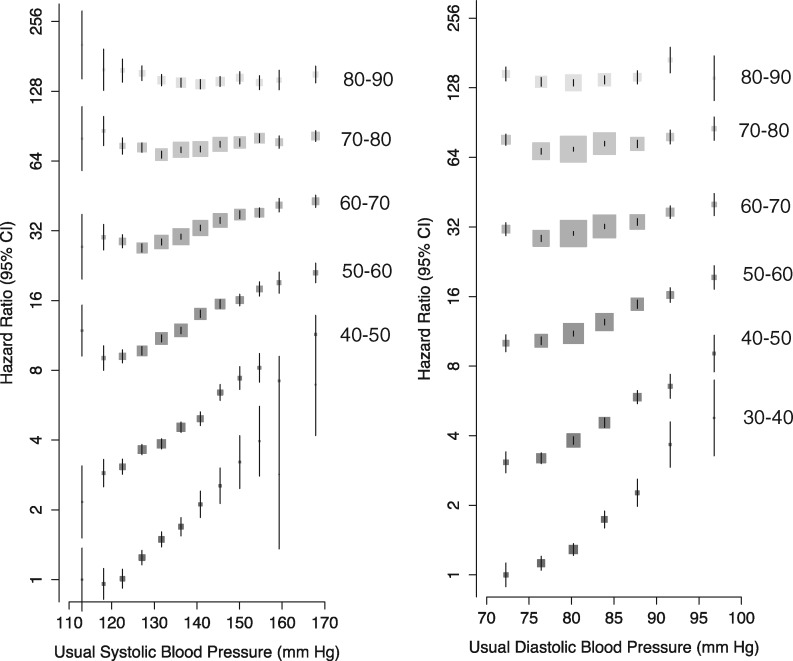
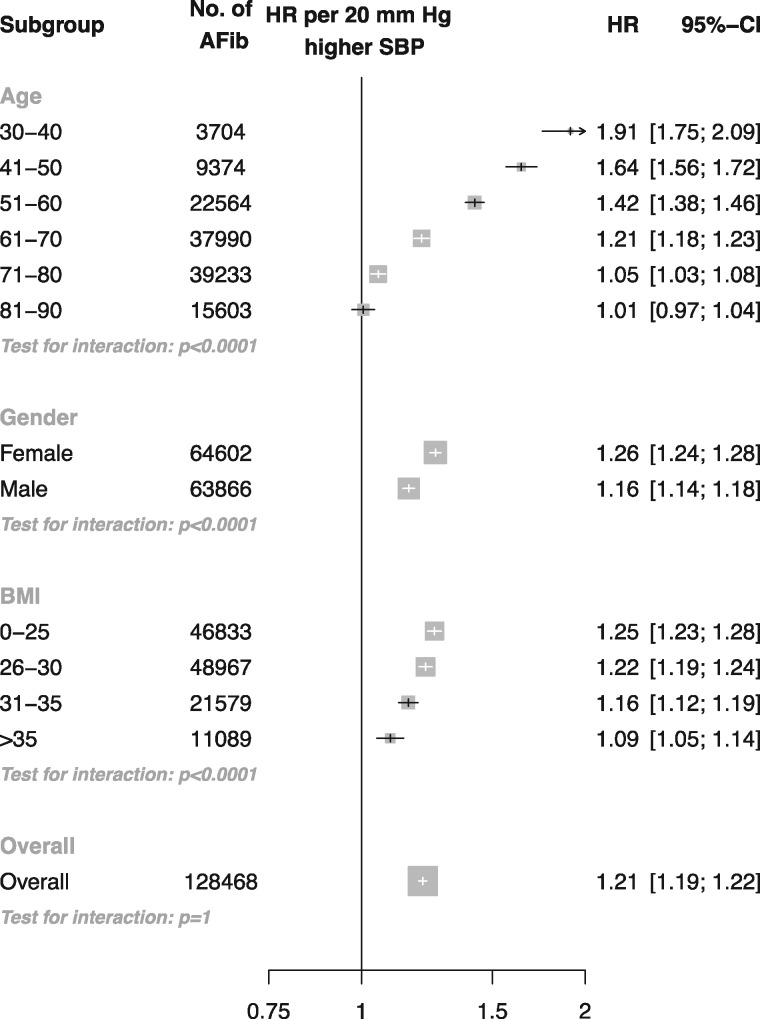
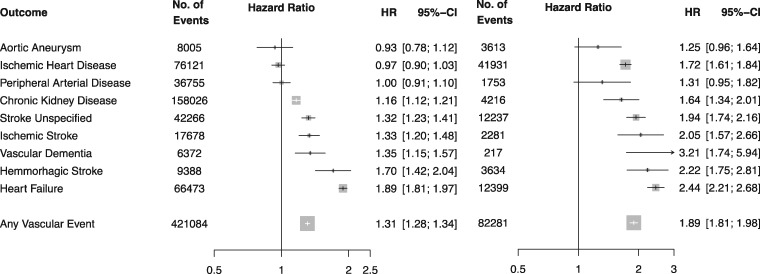
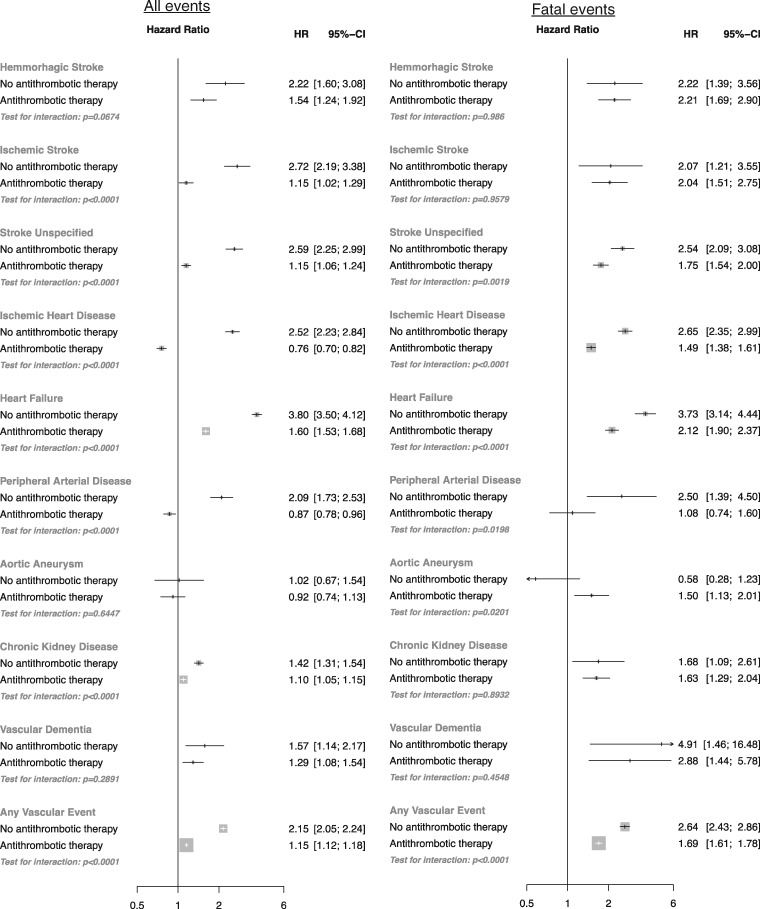
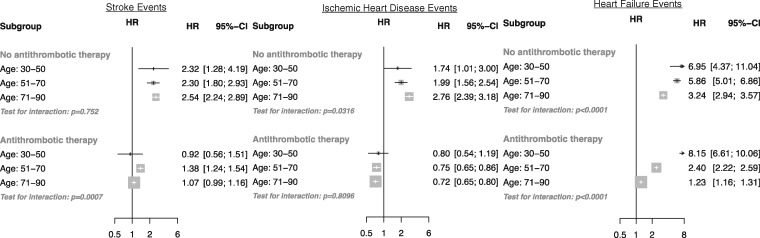
Results: : A 20-mmHg higher usual systolic blood pressure was associated with a higher risk of AF [hazard ratio (HR) 1.21, 95% confidence interval (CI) 1.19, 1.22]. The strength of the association declined with increasing age, from an HR of 1.91 (CI 1.75, 2.09) at age 30-40 to an HR of 1.01 (CI 0.97, 1.04) at age 80-90 years. AF without antithrombotic use at baseline was associated with a greater risk of any vascular event than AF with antithrombotic usage ( P interaction < 0.0001). AF without baseline antithrombotic usage was associated with an increased risk of ischaemic heart disease (HR 2.52, CI 2.23, 2.84), heart failure (HR 3.80, CI 3.50, 4.12), ischaemic stroke (HR 2.72, CI 2.19, 3.38), unspecified stroke (HR 2.59, CI 2.25, 2.99), haemorrhagic stroke, chronic kidney disease, peripheral arterial disease and vascular dementia, but not aortic aneurysm.
Conclusions: The association between elevated blood pressure and AF attenuates with increasing age. AF without antithrombotic usage is associated with an increased risk of eight vascular events.
Keywords: Atrial fibrillation; blood pressure; cardiovascular disease; epidemiology.
© The Author 2016. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ. et al . Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation; 2006;114:119–25. - PubMed
-
- Murray CJL, Vos T, Lozano R. et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197–223. - PubMed
-
- Iwasaki Y-K, Nishida K, Kato T, Nattel S.. Atrial fibrillation pathophysiology: implications for management. Circulation 2011;124:2264–74. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB.. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–88. - PubMed
-
- Thrall G, Lane D, Carroll D, Lip GYH.. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med; 2006;119: 448.e1–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
