

Prognostic Value of Aortic Valve Area by Doppler Echocardiography in Patients With Severe Asymptomatic Aortic Stenosis
- PMID: 27143354
- PMCID: PMC4889185
- DOI: 10.1161/JAHA.115.003146
Prognostic Value of Aortic Valve Area by Doppler Echocardiography in Patients With Severe Asymptomatic Aortic Stenosis
Abstract
Background: The aim of this study was to evaluate the relationship between aortic valve area (AVA) obtained by Doppler echocardiography and outcome in patients with severe asymptomatic aortic stenosis and to define a specific threshold of AVA for identifying asymptomatic patients at very high risk based on their clinical outcome.
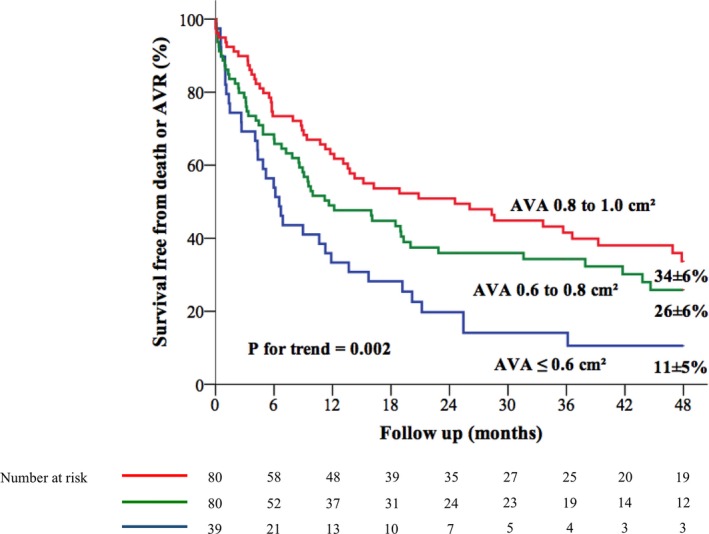
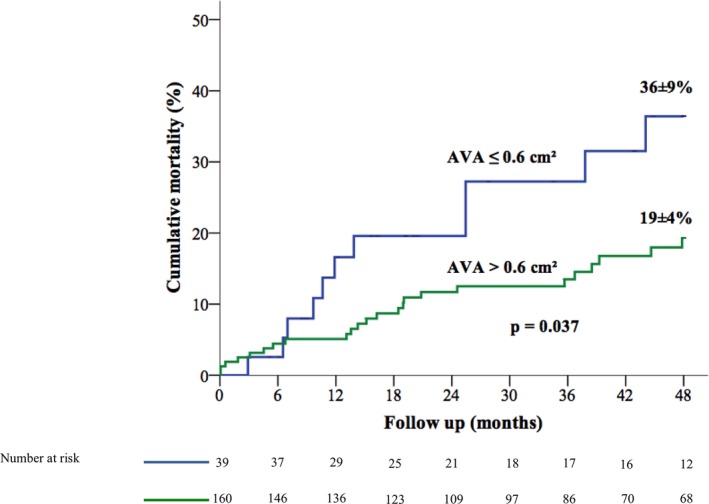
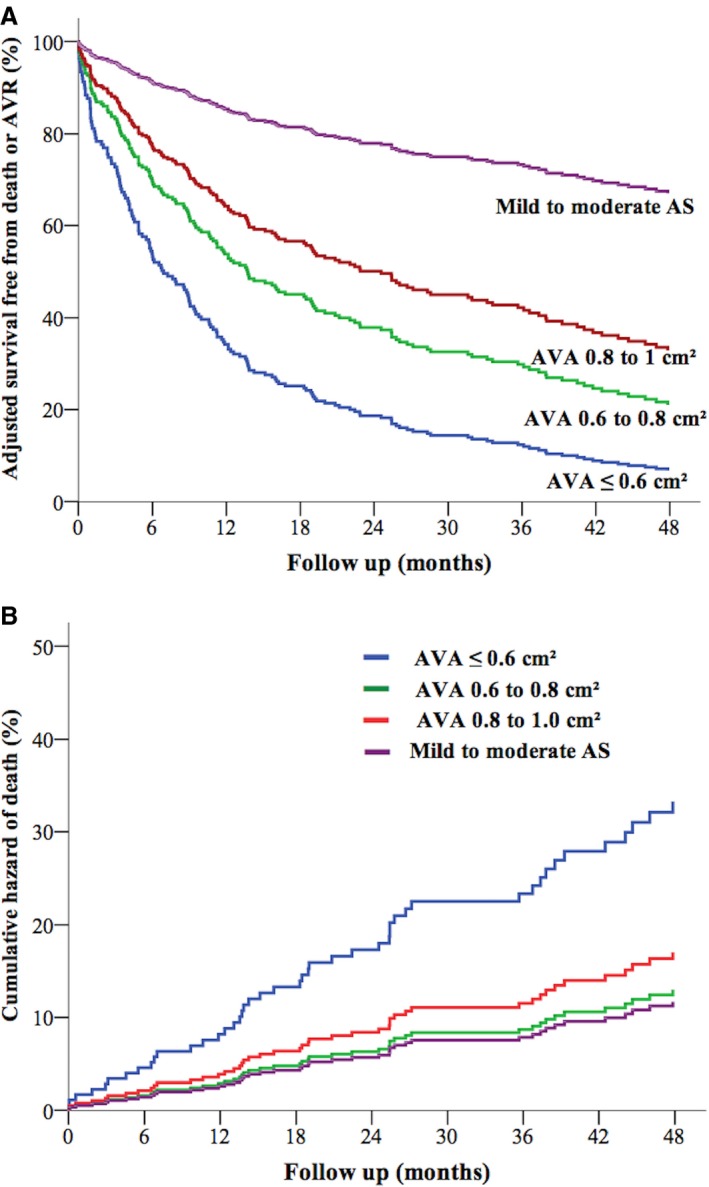
Methods and results: We included 199 patients with asymptomatic severe aortic stenosis (AVA ≤1.0 cm(2)). The risk of events (death or need for aortic valve replacement) increased linearly on the scale of log hazard with decreased AVA (adjusted hazard ratio 1.17; 95% CI 1.06-1.29 per 0.1 cm(2) AVA decrement; P=0.002). Event-free survival at 12, 24, and 48 months was 63±6%, 51±6%, and 34±6%, respectively, for AVA 0.8 to 1 cm(2); 49±6%, 36±6%, and 26±6%, respectively, for AVA 0.6 to 0.8 cm(2); and 33±8%, 20±7%, and 11±5%, respectively, for AVA ≤0.6 cm(2) (Ptrend=0.002). Patients with AVA ≤0.6 cm(2) had a significantly increased risk of events compared with patients with AVA 0.8 to 1 cm(2) (adjusted hazard ratio 2.22; 95% CI 1.41-3.52; P=0.001), whereas patients with AVA 0.6 to 0.8 cm(2) had an increased risk of events compared with those with AVA 0.8 to 1 cm(2), but the difference was not statistically significant (adjusted hazard ratio 1.38; 95% CI 0.93-2.05; P=0.11). After adjustment for covariates and aortic valve replacement as a time-dependent variable, patients with AVA ≤0.6 cm(2) had a significantly greater risk of all-cause mortality than patients with AVA >0.6 cm(2) (hazard ratio 3.39; 95% CI 1.80-6.40; P<0.0001).
Conclusions: Patients with severe asymptomatic aortic stenosis and AVA ≤0.6 cm(2) displayed an important increase in the risk of adverse events during short-term follow-up. Further studies are needed to determine whether elective aortic valve replacement improves outcome in this high-risk subgroup of patients.
Keywords: Doppler echocardiography; aortic stenosis; outcome; surgery.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures


Similar articles
-
Outcome Implication of Aortic Valve Area Normalized to Body Size in Asymptomatic Aortic Stenosis.Circ Cardiovasc Imaging. 2016 Nov;9(11):e005121. doi: 10.1161/CIRCIMAGING.116.005121. Circ Cardiovasc Imaging. 2016. PMID: 27903539
-
Discordant Grading of Aortic Stenosis Severity: Echocardiographic Predictors of Survival Benefit Associated With Aortic Valve Replacement.JACC Cardiovasc Imaging. 2016 Jul;9(7):797-805. doi: 10.1016/j.jcmg.2015.09.026. Epub 2016 May 18. JACC Cardiovasc Imaging. 2016. PMID: 27209111
-
Stress echocardiography to assess stenosis severity and predict outcome in patients with paradoxical low-flow, low-gradient aortic stenosis and preserved LVEF.JACC Cardiovasc Imaging. 2013 Feb;6(2):175-83. doi: 10.1016/j.jcmg.2012.10.015. JACC Cardiovasc Imaging. 2013. PMID: 23489531
-
Watchful waiting care or early intervention in asymptomatic severe aortic stenosis: Where we are.Arch Cardiovasc Dis. 2021 Jan;114(1):59-72. doi: 10.1016/j.acvd.2020.07.002. Epub 2020 Nov 3. Arch Cardiovasc Dis. 2021. PMID: 33153947 Review.
-
Aortic Stenosis Progression: A Systematic Review and Meta-Analysis.JACC Cardiovasc Imaging. 2023 Mar;16(3):314-328. doi: 10.1016/j.jcmg.2022.10.009. Epub 2022 Dec 14. JACC Cardiovasc Imaging. 2023. PMID: 36648053
Cited by
-
Asymptomatic aortic stenosis: An assessment of patients' and of their general practitioners' knowledge, after an indexed specialized assessment in community practice.PLoS One. 2017 Jun 5;12(6):e0178932. doi: 10.1371/journal.pone.0178932. eCollection 2017. PLoS One. 2017. PMID: 28582434 Free PMC article.
-
Severe aortic stenosis is associated with perioperative mortality in proximal femur fracture patients.OTA Int. 2020 May 5;3(2):e054. doi: 10.1097/OI9.0000000000000054. eCollection 2020 Jun. OTA Int. 2020. PMID: 33937694 Free PMC article.
-
Electrocardiographic appearance of aortic stenosis before and after aortic valve replacement.Ann Noninvasive Electrocardiol. 2017 Sep;22(5):e12457. doi: 10.1111/anec.12457. Epub 2017 Apr 21. Ann Noninvasive Electrocardiol. 2017. PMID: 28429500 Free PMC article.
-
Natural history of initially asymptomatic severe aortic stenosis: a one-stage meta-analysis.Clin Res Cardiol. 2025 Mar;114(3):350-367. doi: 10.1007/s00392-024-02465-8. Epub 2024 Jul 15. Clin Res Cardiol. 2025. PMID: 39009912
-
Echocardiographic assessment of aortic stenosis: a practical guideline from the British Society of Echocardiography.Echo Res Pract. 2021 Apr 28;8(1):G19-G59. doi: 10.1530/ERP-20-0035. Echo Res Pract. 2021. PMID: 33709955 Free PMC article.
References
-
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of C, European Association for Cardio‐Thoracic S , Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron‐Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schafers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33:2451–2496. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP III, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM III, Thomas JD; Members AATF . 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–2492. - PubMed
-
- Braunwald E. On the natural history of severe aortic stenosis. J Am Coll Cardiol. 1990;15:1018–1020. - PubMed
-
- Lombard JT, Selzer A. Valvular aortic stenosis. A clinical and hemodynamic profile of patients. Ann Intern Med. 1987;106:292–298. - PubMed
-
- Iung B. Management of asymptomatic aortic stenosis. Heart. 2011;97:253–259. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
