

Human Metapneumovirus Infections Following Hematopoietic Cell Transplantation: Factors Associated With Disease Progression
- PMID: 27143659
- PMCID: PMC4928387
- DOI: 10.1093/cid/ciw284
Human Metapneumovirus Infections Following Hematopoietic Cell Transplantation: Factors Associated With Disease Progression
Abstract
Background: Human metapneumovirus (HMPV) is a newly identified pulmonary pathogen that can cause fatal lower respiratory tract disease (LRD) in hematopoietic cell transplantation (HCT) recipients. Little is known about progression rates from upper respiratory tract infection (URI) to LRD and risk factors associated with progression.
Methods: A total of 118 HCT recipients receiving transplantation between 2004 and 2014 who had HMPV detected in nasopharyngeal, bronchoalveolar lavage, or lung biopsy samples by real-time reverse transcription polymerase chain reaction were retrospectively analyzed.
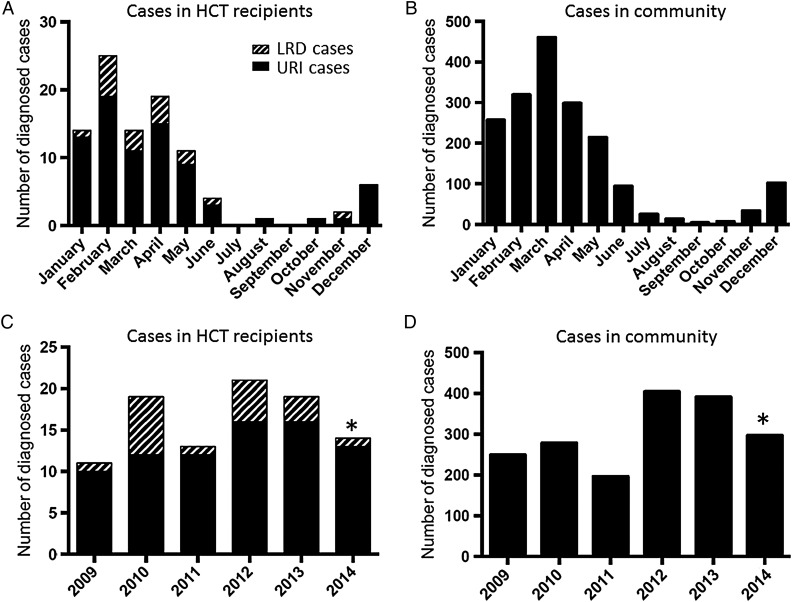
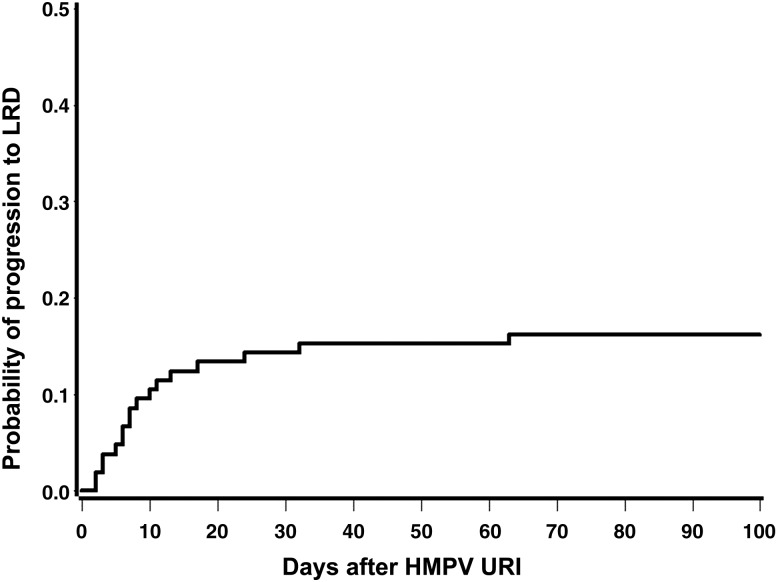
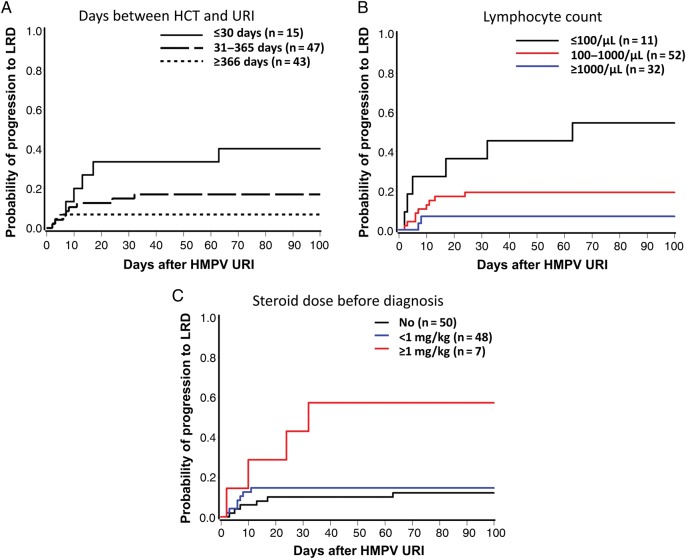
Results: More than 90% of the cases were identified between December and May. Among the 118 HCT patients, 88 and 30 had URI alone and LRD, respectively. Among 30 patients with LRD, 17 patients progressed from URI to LRD after a median of 7 days (range, 2-63 days). The probability of progression to LRD within 40 days after URI was 16%. In Cox regression analysis, steroid use ≥1 mg/kg prior to URI diagnosis (hazard ratio [HR], 5.10; P = .004), low lymphocyte count (HR, 3.43; P = .011), and early onset of HMPV infection after HCT (before day 30 after HCT; HR, 3.54; P = .013) were associated with higher progression to LRD. The median viral load in nasal wash samples was 1.1 × 10(6) copies/mL (range, 3.3 × 10(2)-1.7 × 10(9)) with no correlation between the viral load and progression.
Conclusions: Progression from URI to LRD occurred in up to 60% of HCT recipients with risk factors such as systemic corticosteroid use or low lymphocyte counts. Further studies are needed to define the role of viral load in the pathogenesis of progressive disease.
Keywords: hematopoietic cell transplantation; human metapneumovirus; lower respiratory tract disease; progression.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- Oliveira R, Machado A, Tateno A, Boas LV, Pannuti C, Machado C. Frequency of human metapneumovirus infection in hematopoietic SCT recipients during 3 consecutive years. Bone Marrow Transplant 2008; 42:265–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
