

Biopsychosocial Aspects of Functional Gastrointestinal Disorders
- PMID: 27144624
- PMCID: PMC8809487
- DOI: 10.1053/j.gastro.2016.02.027
Biopsychosocial Aspects of Functional Gastrointestinal Disorders
Abstract
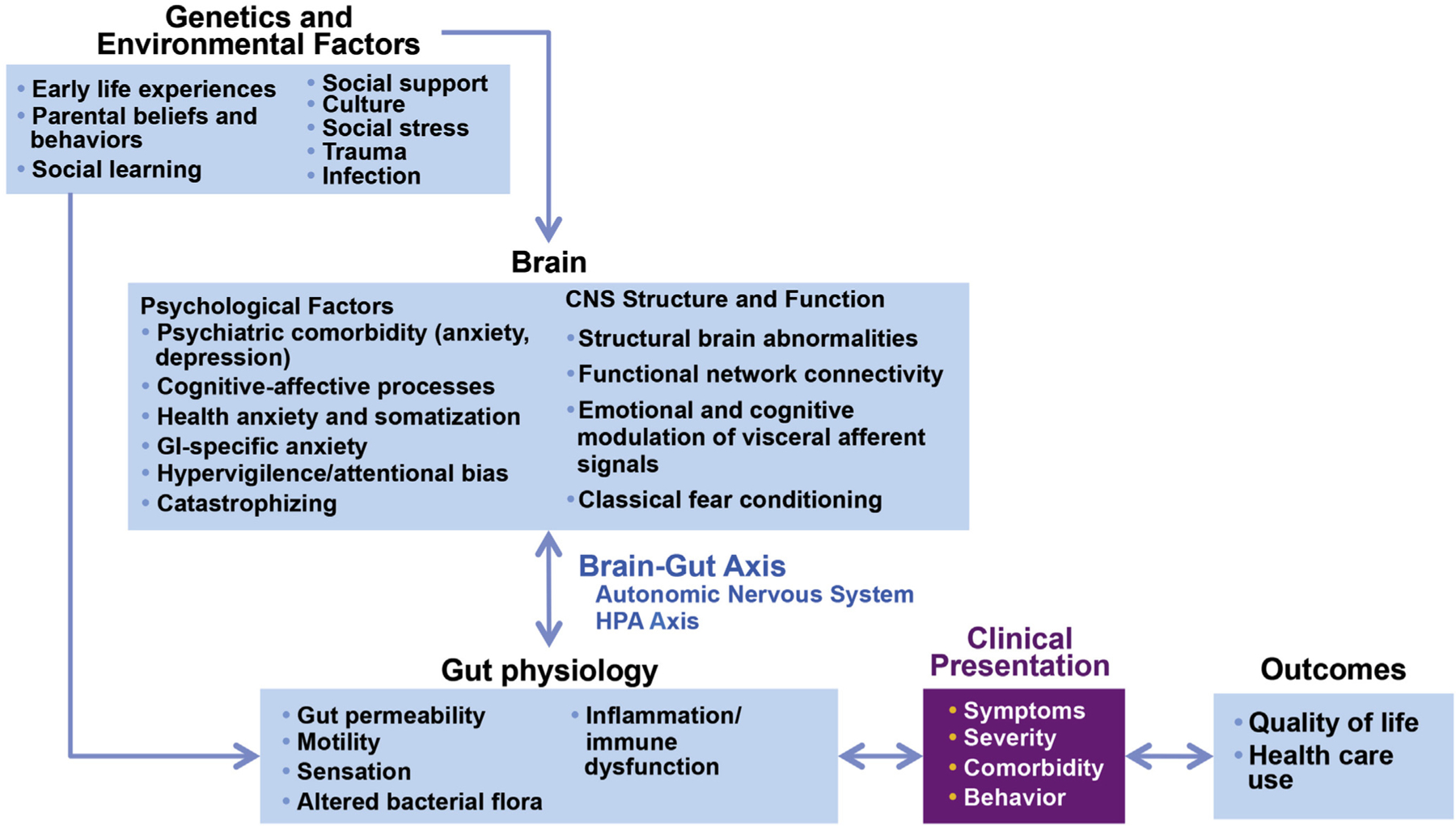
In this paper, we provide a general framework for understanding the functional gastrointestinal disorders (FGID) from a biopsychosocial perspective. More specifically, we provide an overview of the recent research on how the complex interactions of environmental, psychological, and biological factors contribute to the development and maintenance of the FGID. We emphasize that considering and addressing all these factors is a conditio sine qua non for appropriate treatment of these conditions. First, we provide an overview of what is currently known about how each of these factors - the environment, including the influence of those in an individual's family, the individual's own psychological states and traits, and the individual's (neuro)physiological make-up - interact to ultimately result in the generation of FGID symptoms. Second, we provide an overview of commonly used assessment tools which can assist clinicians in obtaining a more comprehensive assessment of these factors in their patients. Finally, the broader perspective outlined earlier is applied to provide an overview of centrally acting treatment strategies, both psychological and pharmacological, which have been shown to be efficacious to treat FGID.
Keywords: Adverse life events; anxiety; cognitive behavioral therapy; depression; exposure treatments; hypnosis; somatic symptom disorder.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
These authors disclose the following: Albena Halpert is on the advisory board of Allergan; Michael Crowell is a consultant for Medtronic-Covidien and Salix. The remaining authors disclose no conflicts.
Figures
References
-
- Bode G, Brenner H, Adler G, Rothenbacher D. Recurrent abdominal pain in children: evidence from a population-based study that social and familial factors play a major role but not Helicobacter pylori infection. J Psychosom Res 2003;54:417–421. - PubMed
-
- Levy RL, Whitehead WE, Von Korff MR, et al. Intergenerational transmission of gastrointestinal illness behavior. Am J Gastroenterol 2000;95:451–456. - PubMed
-
- Walker LS, Garber J, Greene JW. Somatization symptoms in pediatric abdominal pain patients: Relation to chronicity of abdominal pain and parent somatization. J Abnorm Child Psychol 1991;19:379–394. - PubMed
-
- Walker LS, Garber J, Greene JW. Somatic complaints in pediatric patients: a prospective study of the role of negative life events, child social and academic competence, and parental somatic symptoms. J Consult Clin Psychol 1994;62:1213–1221. - PubMed
-
- Levy RL, Jones KR, Whitehead WE, et al. Irritable bowel syndrome in twins: Heredity and social learning both contribute to etiology. Gastroenterology 2001; 121:799–804. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
