

Functional Anorectal Disorders
- PMID: 27144630
- PMCID: PMC5035713
- DOI: 10.1053/j.gastro.2016.02.009
Functional Anorectal Disorders
Abstract
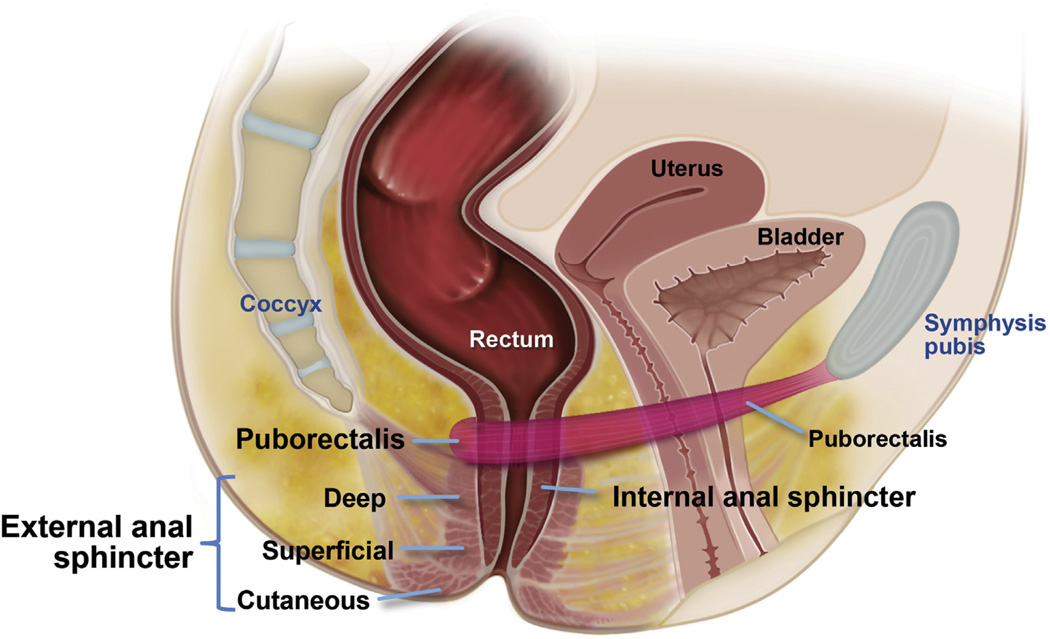
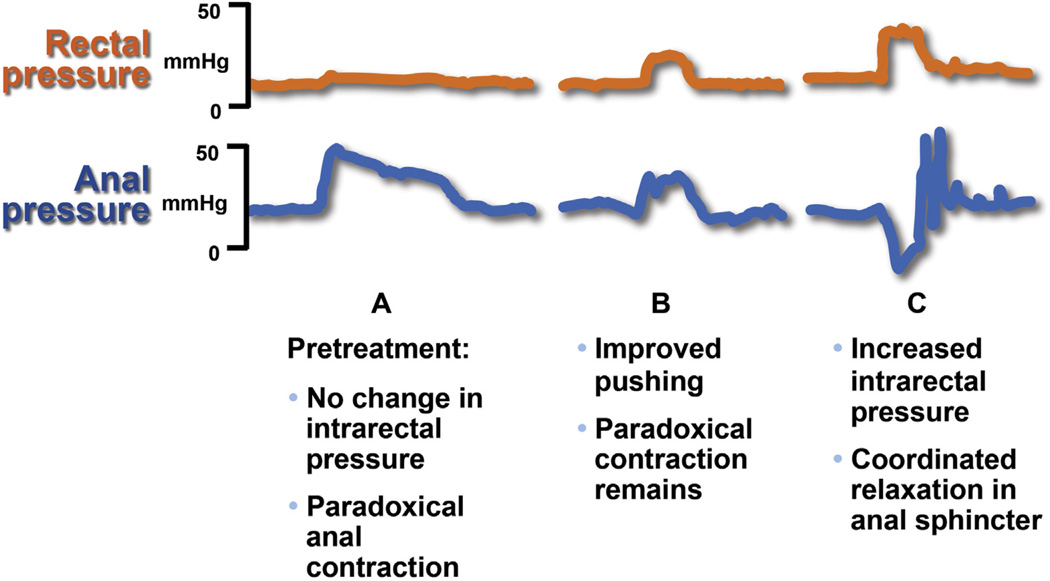
This report defines criteria and reviews the epidemiology, pathophysiology, and management of common anorectal disorders: fecal incontinence (FI), functional anorectal pain and functional defecation disorders. FI is defined as the recurrent uncontrolled passage of fecal material for at least 3 months. The clinical features of FI are useful for guiding diagnostic testing and therapy. Anorectal manometry and imaging are useful for evaluating anal and pelvic floor structure and function. Education, antidiarrheals and biofeedback therapy are the mainstay of management; surgery may be useful in refractory cases. Functional anorectal pain syndromes are defined by clinical features and categorized into three subtypes. In proctalgia fugax, the pain is typically fleeting and lasts for seconds to minutes. In levator ani syndrome (LAS) and unspecified anorectal pain the pain lasts more than 30 minutes, but in LAS there is puborectalis tenderness. Functional defecation disorders are defined by >2 symptoms of chronic constipation or irritable bowel syndrome with constipation, and with >2 features of impaired evacuation i.e., abnormal evacuation pattern on manometry, abnormal balloon expulsion test or impaired rectal evacuation by imaging. It includes two subtypes; dyssynergic defecation and inadequate defecatory propulsion. Pelvic floor biofeedback therapy is effective for treating LAS and defecatory disorders.
Keywords: Anorectal disorders; Anorectal pain; Biofeedback therapy; Constipation; Dyssynergic defecation; Fecal incontinence; Levator ani syndrome.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose the following: AEB is an inventor of the portable anorectal manometry catheter that has been licensed to Medspira Inc; AEB and Mayo Clinic have contractual rights to receive royalties from the licensing of this technology. GC is an advisory board member and speaker for Shire Italia and Takeda Italia. The remaining authors disclose no conflicts.
Figures
References
-
- Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal disorders. Gastroenterology. 2006;130:1510–1518. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
