

BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants
- PMID: 27146380
- PMCID: PMC4856854
- DOI: 10.1136/bmj.i2156
BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants
Abstract
Objective: To conduct a systematic review and meta-analysis of cohort studies of body mass index (BMI) and the risk of all cause mortality, and to clarify the shape and the nadir of the dose-response curve, and the influence on the results of confounding from smoking, weight loss associated with disease, and preclinical disease.
Data sources: PubMed and Embase databases searched up to 23 September 2015.
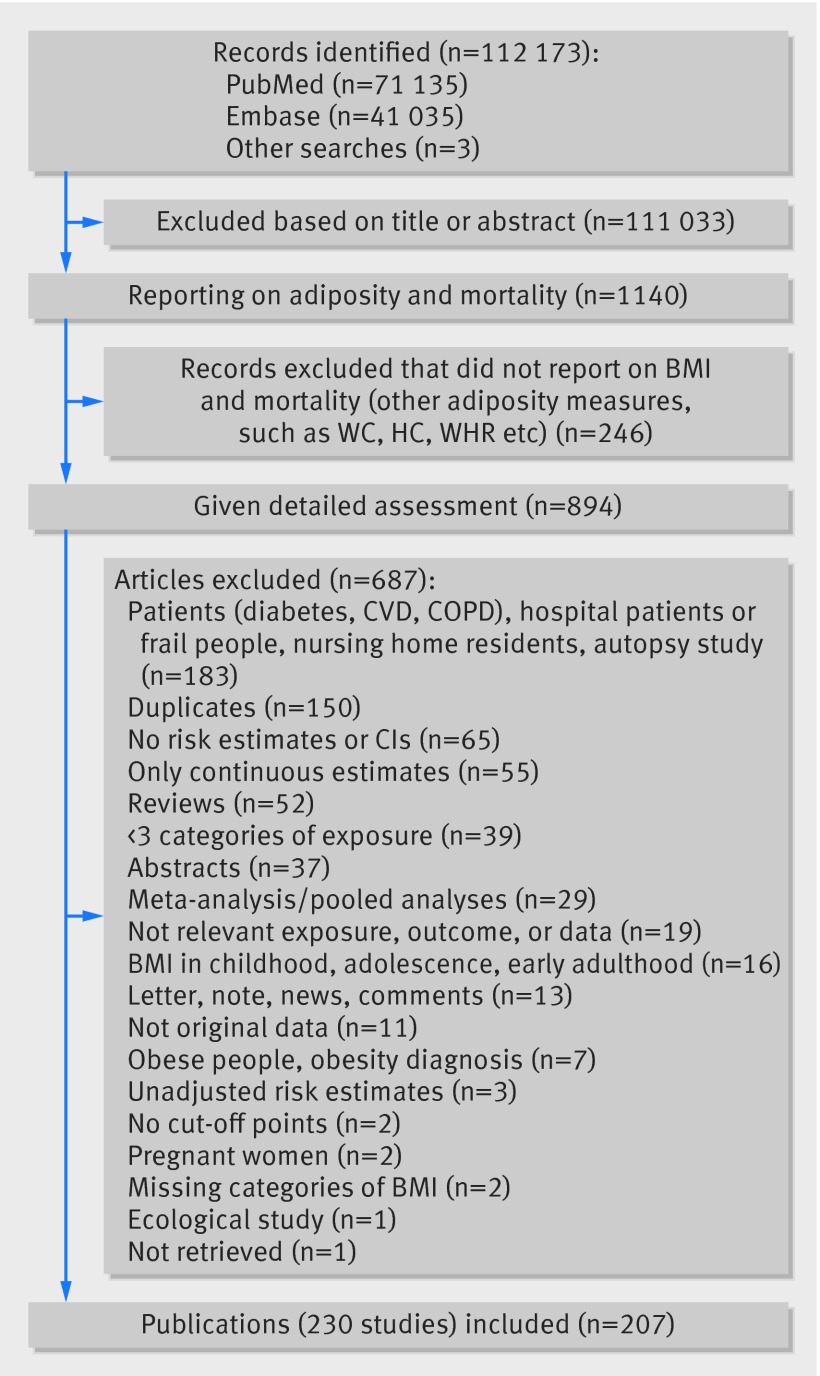
Study selection: Cohort studies that reported adjusted risk estimates for at least three categories of BMI in relation to all cause mortality.
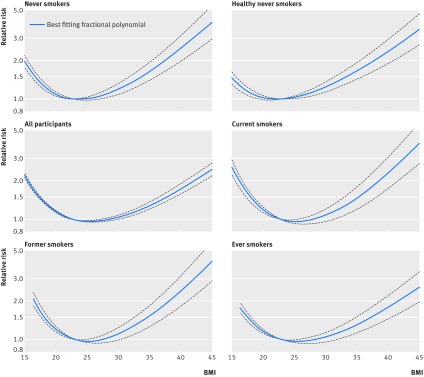
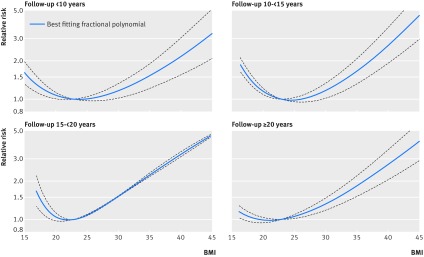
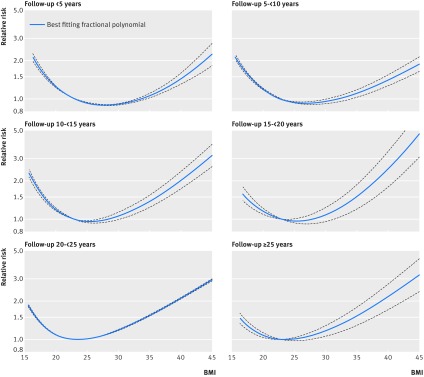
Data synthesis: Summary relative risks were calculated with random effects models. Non-linear associations were explored with fractional polynomial models.
Results: 230 cohort studies (207 publications) were included. The analysis of never smokers included 53 cohort studies (44 risk estimates) with >738 144 deaths and >9 976 077 participants. The analysis of all participants included 228 cohort studies (198 risk estimates) with >3 744 722 deaths among 30 233 329 participants. The summary relative risk for a 5 unit increment in BMI was 1.18 (95% confidence interval 1.15 to 1.21; I(2)=95%, n=44) among never smokers, 1.21 (1.18 to 1.25; I(2)=93%, n=25) among healthy never smokers, 1.27 (1.21 to 1.33; I(2)=89%, n=11) among healthy never smokers with exclusion of early follow-up, and 1.05 (1.04 to 1.07; I(2)=97%, n=198) among all participants. There was a J shaped dose-response relation in never smokers (Pnon-linearity <0.001), and the lowest risk was observed at BMI 23-24 in never smokers, 22-23 in healthy never smokers, and 20-22 in studies of never smokers with ≥20 years' follow-up. In contrast there was a U shaped association between BMI and mortality in analyses with a greater potential for bias including all participants, current, former, or ever smokers, and in studies with a short duration of follow-up (<5 years or <10 years), or with moderate study quality scores.
Conclusion: Overweight and obesity is associated with increased risk of all cause mortality and the nadir of the curve was observed at BMI 23-24 among never smokers, 22-23 among healthy never smokers, and 20-22 with longer durations of follow-up. The increased risk of mortality observed in underweight people could at least partly be caused by residual confounding from prediagnostic disease. Lack of exclusion of ever smokers, people with prevalent and preclinical disease, and early follow-up could bias the results towards a more U shaped association.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Body mass index and mortality: understanding the patterns and paradoxes.BMJ. 2016 May 4;353:i2433. doi: 10.1136/bmj.i2433. BMJ. 2016. PMID: 27146663 No abstract available.
Comment on
-
Methods for trend estimation from summarized dose-response data, with applications to meta-analysis.Am J Epidemiol. 1992 Jun 1;135(11):1301-9. doi: 10.1093/oxfordjournals.aje.a116237. Am J Epidemiol. 1992. PMID: 1626547
-
Meta-analysis in clinical trials.Control Clin Trials. 1986 Sep;7(3):177-88. doi: 10.1016/0197-2456(86)90046-2. Control Clin Trials. 1986. PMID: 3802833
References
-
- Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014;384:766-81. 10.1016/S0140-6736(14)60460-8 pmid:24880830. - DOI - PMC - PubMed
-
- Whitlock G, Lewington S, Sherliker P, et al. Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 2009;373:1083-96. 10.1016/S0140-6736(09)60318-4 pmid:19299006. - DOI - PMC - PubMed
-
- Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract 2010;89:309-19. 10.1016/j.diabres.2010.04.012 pmid:20493574. - DOI - PubMed
-
- World Cancer Research Fund/American Insitute for Cancer Research. Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective.AICR, 2007.
-
- Aune D, Greenwood DC, Chan DS, et al. Body mass index, abdominal fatness and pancreatic cancer risk: a systematic review and non-linear dose-response meta-analysis of prospective studies. Ann Oncol 2012;23:843-52. 10.1093/annonc/mdr398 pmid:21890910. - DOI - PubMed