

Pattern and Prognostic Implications of Cardiac Metastases Among Patients With Advanced Systemic Cancer Assessed With Cardiac Magnetic Resonance Imaging
- PMID: 27146445
- PMCID: PMC4889201
- DOI: 10.1161/JAHA.116.003368
Pattern and Prognostic Implications of Cardiac Metastases Among Patients With Advanced Systemic Cancer Assessed With Cardiac Magnetic Resonance Imaging
Abstract
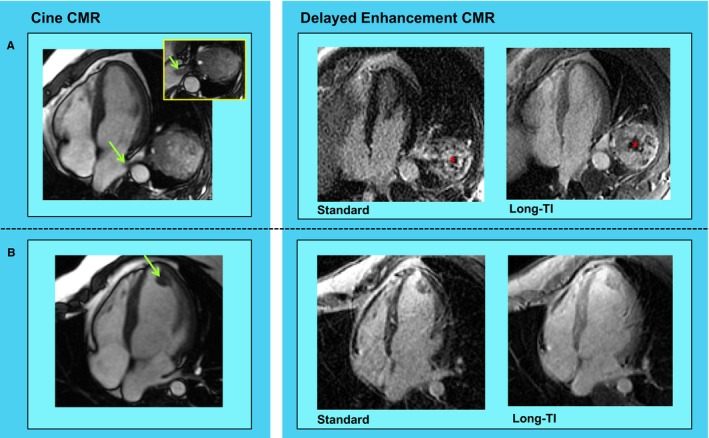
Background: Cardiac magnetic resonance (CMR) imaging is well validated for tissue characterization of cardiac masses but has not been applied to study pattern and prognostic implications of cardiac metastases (CMETs) among patients with systemic cancer.
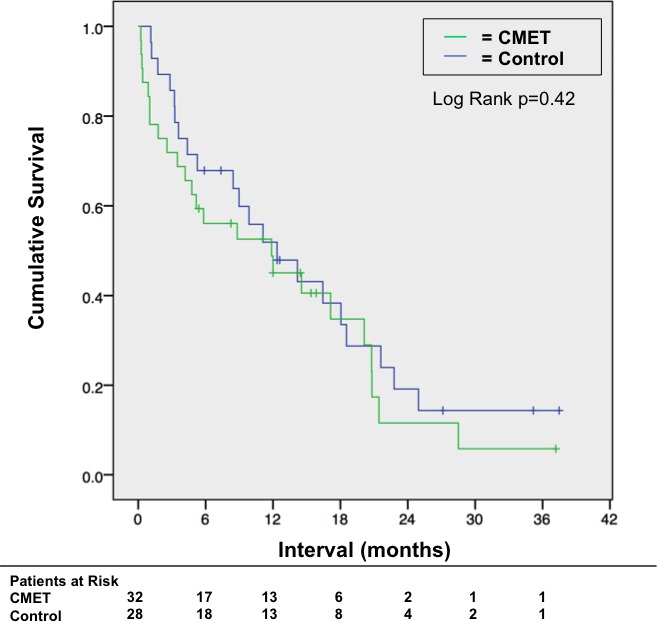
Methods and results: The population consisted of 60 patients with stage IV cancer (32 patients with CMETs, 28 diagnosis-matched controls) undergoing CMR. CMET was defined as a discrete mass with vascular tissue properties on delayed enhancement CMR. CMET-positive patients and controls had similar clinical characteristics, cardiac geometry, and function (P=NS). Leading cancer types associated with CMET were sarcoma, melanoma, and gastrointestinal. Patients with CMETs had similar distribution of extracardiac metastatic disease compared with controls (organs involved: 3.4±2.0 versus 2.7±1.9, P=0.17). In 94% of patients with CMETs, there were metastases involving ≥1 extracardiac organ (66% lung involvement). CMET location varied (right ventricle 44%, right atrium 19%, left ventricle 28%, left atrium 9%, pericardial 25%); 22% of cases had multichamber involvement. Right-sided chamber involvement was common in hematologic/lymphatic spread (67%); pericardial involvement was common with direct spread (64%). Regarding tissue properties on delayed enhancement CMR, CMETs commonly (59%) demonstrated heterogeneous enhancement (41% diffuse enhancement). Heterogeneous lesions were larger and had increased border irregularity (P<0.05). Survival 6 months post-CMR was numerically lower among patients with CMETs (56% [95% CI 39-74%]) versus stage IV cancer-matched controls (68% [95% CI 50-86%]), although differences between groups were nonsignificant (P=0.42).
Conclusions: CMETs vary regarding etiology, location, and tissue properties on CMR, highlighting need for comprehensive surveillance of cardiac involvement regardless of cancer origin. Prognosis remains poor with for patients with CMETs, albeit similar to that for stage IV cancer controls matched for cancer etiology.
Keywords: cardiac metastases; cardiac tumor; cardiovascular magnetic resonance; cardio‐oncology; oncology.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Klatt EC, Heitz DR. Cardiac metastases. Cancer. 1990;65:1456–1459. - PubMed
-
- Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20‐year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993;117:1027–1031. - PubMed
-
- Weinsaft JW, Kim RJ, Ross M, Krauser D, Manoushagian S, LaBounty TM, Cham MD, Min JK, Healy K, Wang Y, Parker M, Roman MJ, Devereux RB. Contrast‐enhanced anatomic imaging as compared with contrast‐enhanced tissue characterization for detection of left ventricular thrombus. JACC Cardiovasc Imaging. 2009;2:969–979. - PMC - PubMed
-
- Weinsaft JW, Kim HW, Crowley AL, Klem I, Shenoy C, Van Assche L, Brosnan R, Shah DJ, Velazquez EJ, Parker M, Judd RM, Kim RJ. LV thrombus detection by routine echocardiography: insights into performance characteristics using delayed enhancement CMR. JACC Cardiovasc Imaging. 2011;4:702–712. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
