

Physiologic Reelin does not play a strong role in protection against acute stroke
- PMID: 27146512
- PMCID: PMC4929708
- DOI: 10.1177/0271678X16646386
Physiologic Reelin does not play a strong role in protection against acute stroke
Abstract
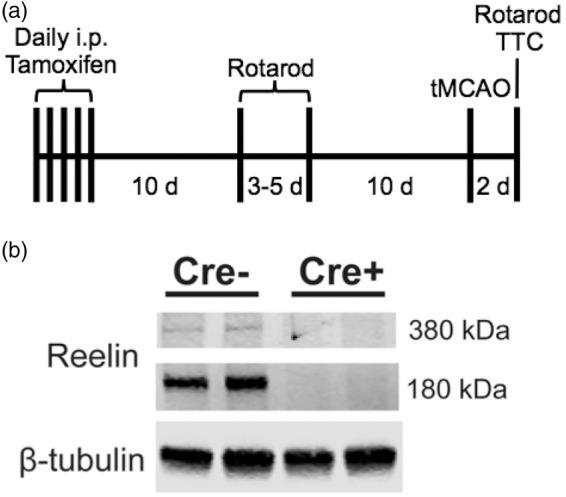
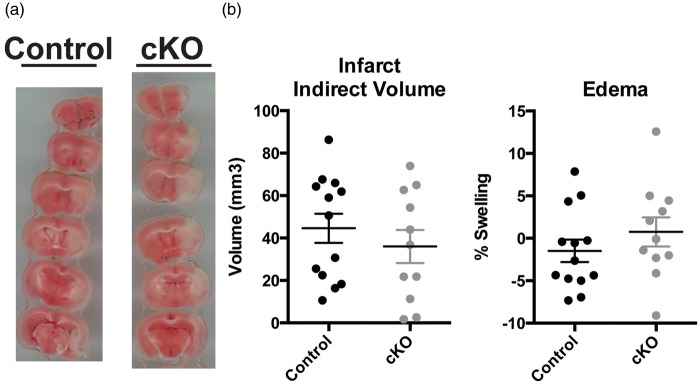
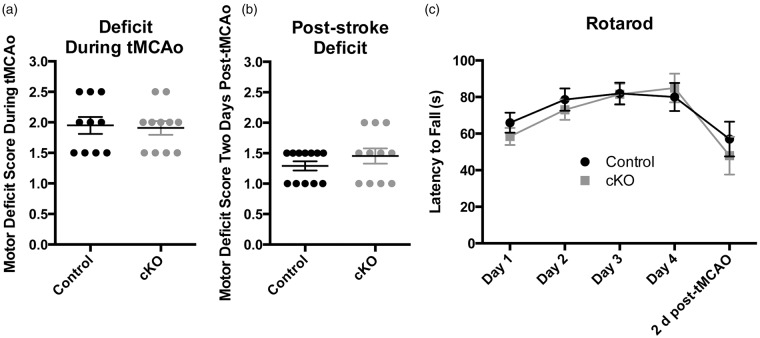
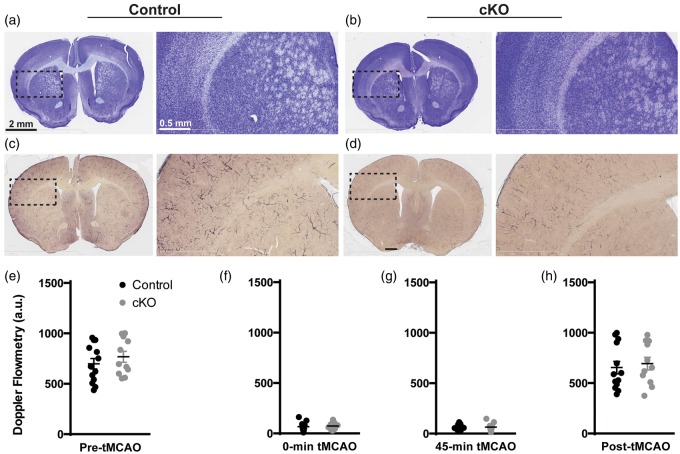
Stroke and Alzheimer's disease, two diseases that disproportionately affect the aging population, share a subset of pathological findings and risk factors. The primary genetic risk factor after age for late-onset Alzheimer's disease, ApoE4, has also been shown to increase stroke risk and the incidence of post-stroke dementia. One mechanism by which ApoE4 contributes to disease is by inducing in neurons a resistance to Reelin, a neuromodulator that enhances synaptic function. Previous studies in Reelin knockout mice suggest a role for Reelin in protection against stroke; however, these studies were limited by the developmental requirement for Reelin in neuronal migration. To address the question of the effect of Reelin loss on stroke susceptibility in an architecturally normal brain, we utilized a novel mouse with induced genetic reduction of Reelin. We found that after transient middle cerebral artery occlusion, mice with complete adult loss of Reelin exhibited a similar level of functional deficit and extent of infarct as control mice. Together, these results suggest that physiological Reelin does not play a strong role in protection against stroke pathology.
Keywords: ApoE4; Reelin; Reelin conditional knockout; stroke; transient middle cerebral artery occlusion.
© The Author(s) 2016.
Figures
References
-
- Alzheimer's A. 2014 Alzheimer's disease facts and figures. Alzheimers Dement 2014; 10: e47–e92. - PubMed
-
- Snowdon DA, Greiner LH, Mortimer JA, et al. Brain infarction and the clinical expression of Alzheimer disease. The Nun Study. JAMA 1997; 277: 813–817. - PubMed
-
- Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol 2009; 8: 1006–1018. - PubMed
-
- Hiltunen M, Makinen P, Peraniemi S, et al. Focal cerebral ischemia in rats alters APP processing and expression of Abeta peptide degrading enzymes in the thalamus. Neurobiol Dis 2009; 35: 103–1. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
