

Risk prediction for local versus regional/metastatic tumors after initial ductal carcinoma in situ diagnosis treated by lumpectomy
- PMID: 27146587
- PMCID: PMC6805143
- DOI: 10.1007/s10549-016-3814-z
Risk prediction for local versus regional/metastatic tumors after initial ductal carcinoma in situ diagnosis treated by lumpectomy
Abstract
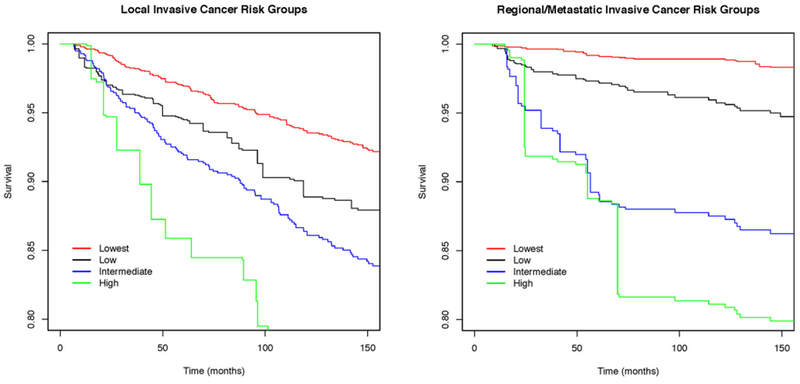
Among women diagnosed with ductal carcinoma in situ (DCIS), we identified factors associated with local invasive cancer (LIC) and regional/metastatic invasive cancer (RMIC) and provide 10-year risks based on clinically relevant factors. We created a retrospective, population-based cohort of 1492 women with an initial diagnosis of DCIS (1983-1996) treated by lumpectomy alone. Histological and molecular markers (Ki67, ER, PR, COX-2, p16, ERBB2) were collected on DCIS cases with a subsequent tumor (DCIS, LIC, or RMIC) and a subsample of frequency-matched controls without subsequent tumors. Competing risks methods were used to identify factors associated with LIC and RMIC and cumulative incidence methods to estimate 10-year risks for combinations of factors. Median follow-up time was 12.6 years (range 0.5-29.5 years). The overall 10-year risk of LIC (11.9 %) was higher than for RMIC (3.8 %). About half of women with initial DCIS lesions are detected by mammography and p16 negative and have a 10-year risk of LIC of 6.2 % (95 % CI 5.8-6.8 %) and RMIC of 1.2 % (95 % CI 1.1-1.3 %). Premenopausal women whose DCIS lesion was p16 positive or p16 negative and detected by palpation had high 10-year risk of LIC of 23.0 % (95 % CI 19.3-27.4 %). Ten-year risk of RMIC was highest at 22.5 % (95 % CI 13.8-48.1 %) for those positive for p16, COX-2, and ERRB2, and negative for ER, but prevalence of this group is low at 3 %. Ten-year risk of LIC and RMIC is low for the majority diagnosed with DCIS. Combinations of molecular markers and method of detection of initial DCIS lesion can differentiate women at low and high risk of LIC and RMIC.
Keywords: Ductal carcinoma in situ; Local invasive cancer; Recurrence; Regional/metastatic invasive cancer; Risk.
Conflict of interest statement
Compliance with ethical standards
Figures
Similar articles
-
Biomarker expression and risk of subsequent tumors after initial ductal carcinoma in situ diagnosis.J Natl Cancer Inst. 2010 May 5;102(9):627-37. doi: 10.1093/jnci/djq101. Epub 2010 Apr 28. J Natl Cancer Inst. 2010. PMID: 20427430 Free PMC article.
-
Characteristics associated with recurrence among women with ductal carcinoma in situ treated by lumpectomy.J Natl Cancer Inst. 2003 Nov 19;95(22):1692-702. doi: 10.1093/jnci/djg097. J Natl Cancer Inst. 2003. PMID: 14625260
-
Ten-year risk of diagnostic mammograms and invasive breast procedures after breast-conserving surgery for DCIS.J Natl Cancer Inst. 2012 Apr 18;104(8):614-21. doi: 10.1093/jnci/djs167. Epub 2012 Apr 5. J Natl Cancer Inst. 2012. PMID: 22491230 Free PMC article.
-
Ductal carcinoma in situ, complexities and challenges.J Natl Cancer Inst. 2004 Jun 16;96(12):906-20. doi: 10.1093/jnci/djh164. J Natl Cancer Inst. 2004. PMID: 15199110 Review.
-
[The treatment of ductal carcinoma in situ (DCIS) of the breast].Ned Tijdschr Geneeskd. 2003 Nov 1;147(44):2157-61. Ned Tijdschr Geneeskd. 2003. PMID: 14626831 Review. Dutch.
Cited by
-
A living biobank of patient-derived ductal carcinoma in situ mouse-intraductal xenografts identifies risk factors for invasive progression.Cancer Cell. 2023 May 8;41(5):986-1002.e9. doi: 10.1016/j.ccell.2023.04.002. Epub 2023 Apr 27. Cancer Cell. 2023. PMID: 37116492 Free PMC article.
-
Comparative effectiveness of incorporating a hypothetical DCIS prognostic marker into breast cancer screening.Breast Cancer Res Treat. 2018 Feb;168(1):229-239. doi: 10.1007/s10549-017-4582-0. Epub 2017 Nov 28. Breast Cancer Res Treat. 2018. PMID: 29185118 Free PMC article.
-
Immune cell infiltrate in ductal carcinoma in situ and the risk of dying from breast cancer: case-control study.Br J Surg. 2024 Jan 31;111(2):znae037. doi: 10.1093/bjs/znae037. Br J Surg. 2024. PMID: 38395442 Free PMC article.
-
Loss of myoepithelial calponin-1 characterizes high-risk ductal carcinoma in situ cases, which are further stratified by T cell composition.Mol Carcinog. 2020 Jul;59(7):701-712. doi: 10.1002/mc.23171. Epub 2020 Mar 5. Mol Carcinog. 2020. PMID: 32134153 Free PMC article.
-
Ductal Carcinoma In Situ Biology, Biomarkers, and Diagnosis.Front Oncol. 2017 Oct 23;7:248. doi: 10.3389/fonc.2017.00248. eCollection 2017. Front Oncol. 2017. PMID: 29109942 Free PMC article. Review.
References
-
- Siegel R, Miller K, Jemal A (2015) Cancer statistics, 2015. CA Cancer J Clin 65(1):5–29 - PubMed
-
- American Cancer Society (2013) Breast cancer facts & figures (2013-2014) In: American Cancer Society, Inc, Atlanta
-
- Ernster VL, Ballard-Barbash R, Barlow WE, Zheng Y, Weaver DL, Cutter G, Yankaskas BC, Rosenberg R, Carney PA, Kerlikowske K et al. (2002) Detection of ductal carcinoma in situ in women undergoing screening mammography. J Natl Cancer Inst 94(20):1546–1554 - PubMed
-
- Virnig BA, Tuttle TM, Shamliyan T, Kane RL (2010) Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. JNCI 102(3):170–178 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
