

A new prognostic histopathologic classification of nasopharyngeal carcinoma
- PMID: 27146632
- PMCID: PMC4857443
- DOI: 10.1186/s40880-016-0103-5
A new prognostic histopathologic classification of nasopharyngeal carcinoma
Abstract
Background: The current World Health Organization (WHO) classification of nasopharyngeal carcinoma (NPC) conveys little prognostic information. This study aimed to propose an NPC histopathologic classification that can potentially be used to predict prognosis and treatment response.
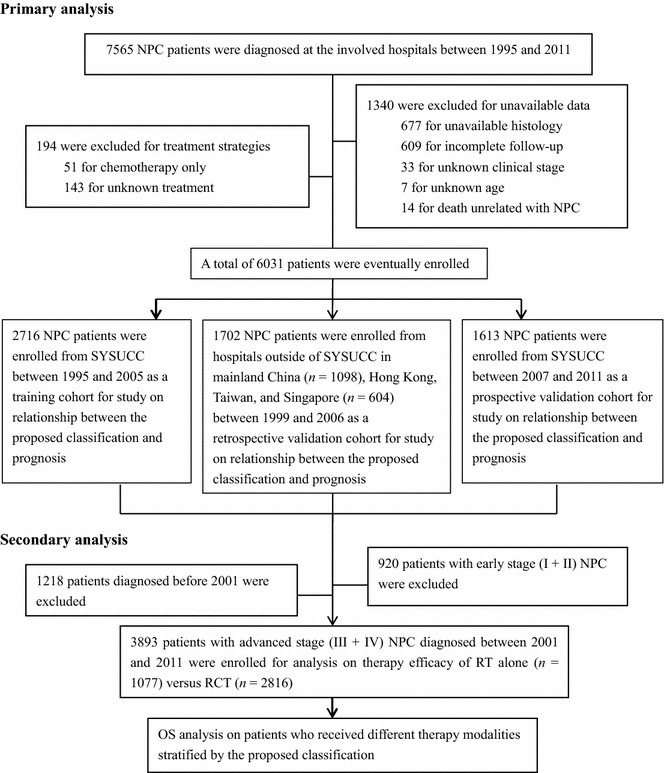
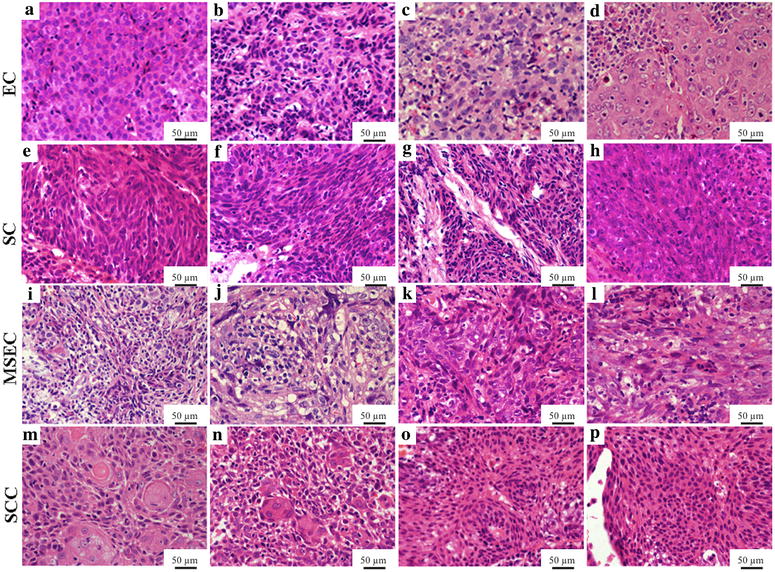
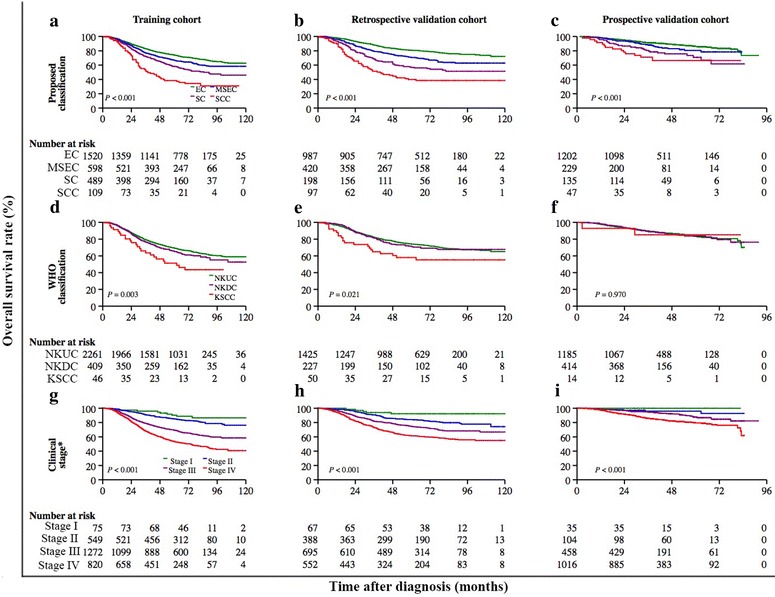
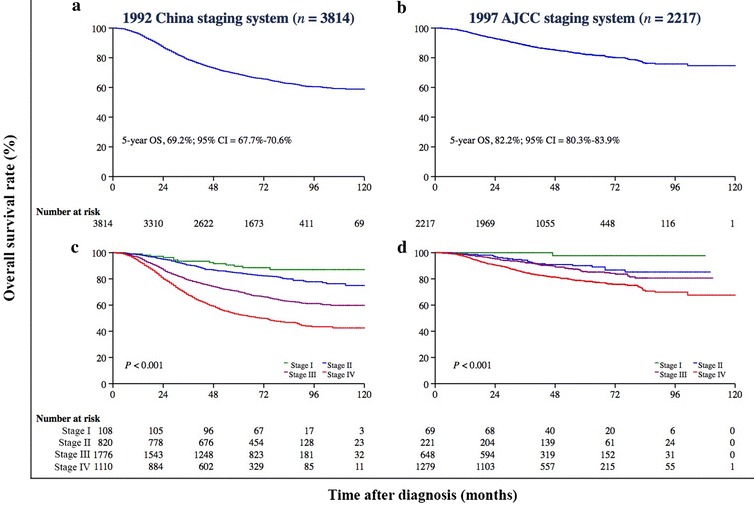
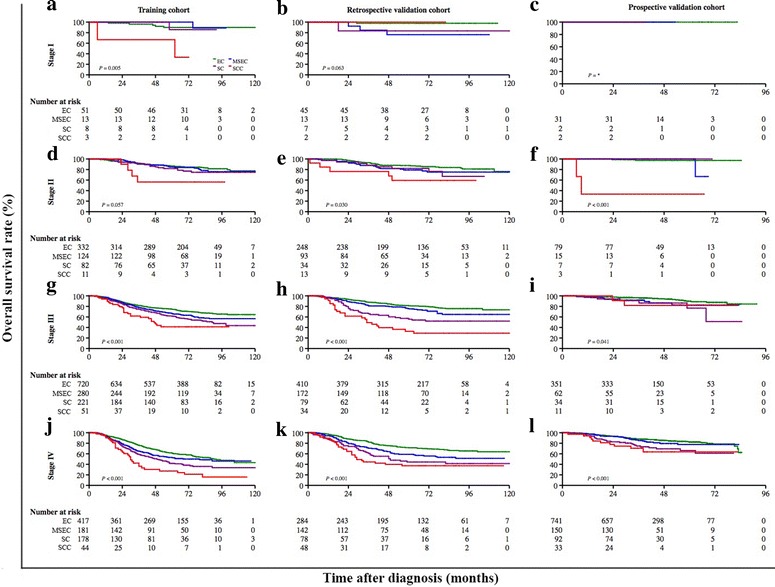
Methods: We initially developed a histopathologic classification based on the morphologic traits and cell differentiation of tumors of 2716 NPC patients who were identified at Sun Yat-sen University Cancer Center (SYSUCC) (training cohort). Then, the proposed classification was applied to 1702 patients (retrospective validation cohort) from hospitals outside SYSUCC and 1613 patients (prospective validation cohort) from SYSUCC. The efficacy of radiochemotherapy and radiotherapy modalities was compared between the proposed subtypes. We used Cox proportional hazards models to estimate hazard ratios (HRs) with 95% confidence intervals (CI) for overall survival (OS).
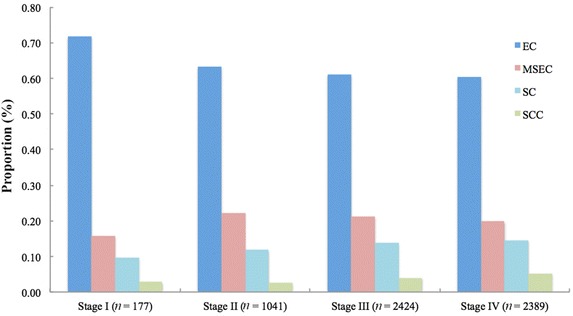
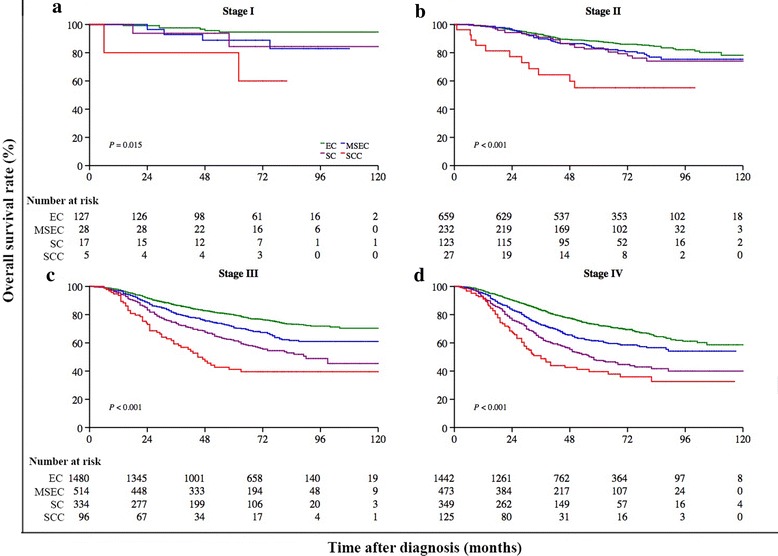
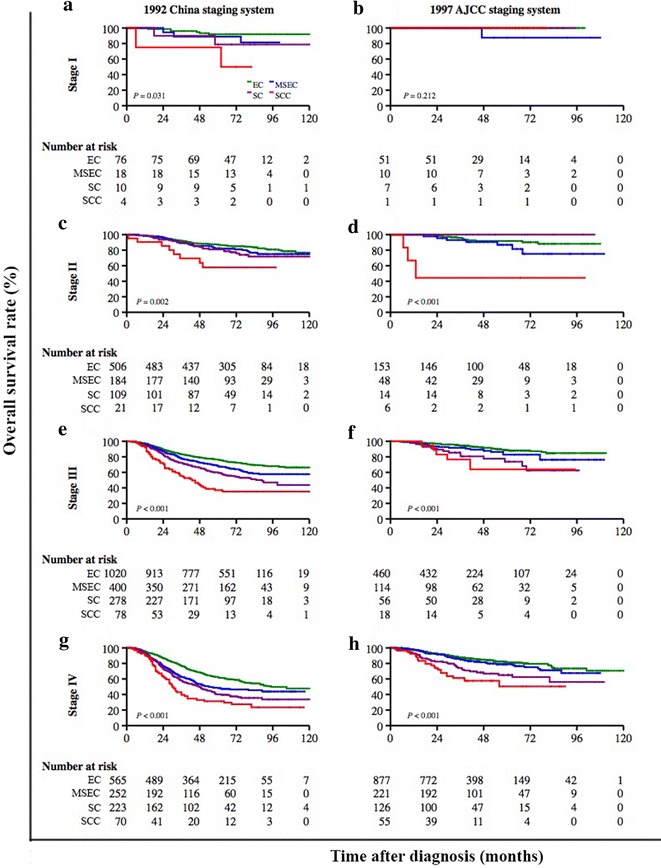
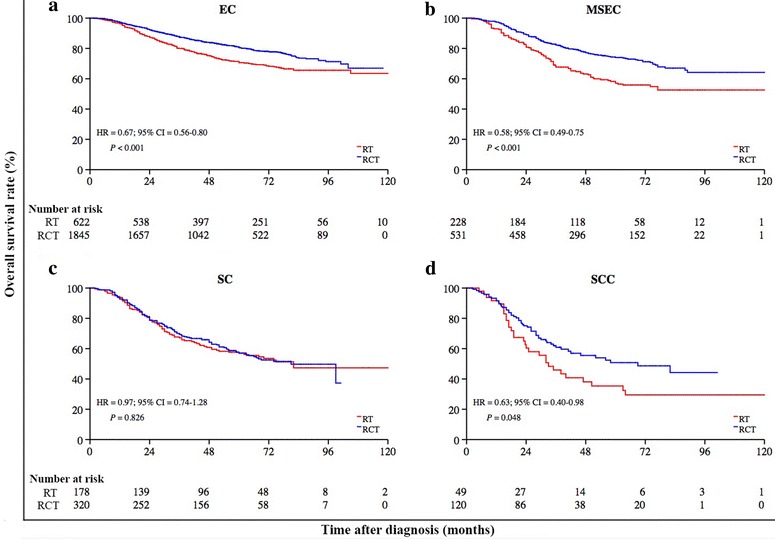
Results: The 5-year OS rates for all NPC patients who were diagnosed with epithelial carcinoma (EC; 3708 patients), mixed sarcomatoid-epithelial carcinoma (MSEC; 1247 patients), sarcomatoid carcinoma (SC; 823 patients), and squamous cell carcinoma (SCC; 253 patients) were 79.4%, 70.5%, 59.6%, and 42.6%, respectively (P < 0.001). In multivariate models, patients with MSEC had a shorter OS than patients with EC (HR = 1.44, 95% CI = 1.27-1.62), SC (HR = 2.00, 95% CI = 1.76-2.28), or SCC (HR = 4.23, 95% CI = 3.34-5.38). Radiochemotherapy significantly improved survival compared with radiotherapy alone for patients with EC (HR = 0.67, 95% CI = 0.56-0.80), MSEC (HR = 0.58, 95% CI = 0.49-0.75), and possibly for those with SCC (HR = 0.63; 95% CI = 0.40-0.98), but not for patients with SC (HR = 0.97, 95% CI = 0.74-1.28).
Conclusions: The proposed classification offers more information for the prediction of NPC prognosis compared with the WHO classification and might be a valuable tool to guide treatment decisions for subtypes that are associated with a poor prognosis.
Keywords: Nasopharyngeal carcinoma; Pathologic classification; Prognosis.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
