Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B
- PMID: 27146801
- PMCID: PMC4857102
- DOI: 10.1038/srep25487
Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B
Abstract
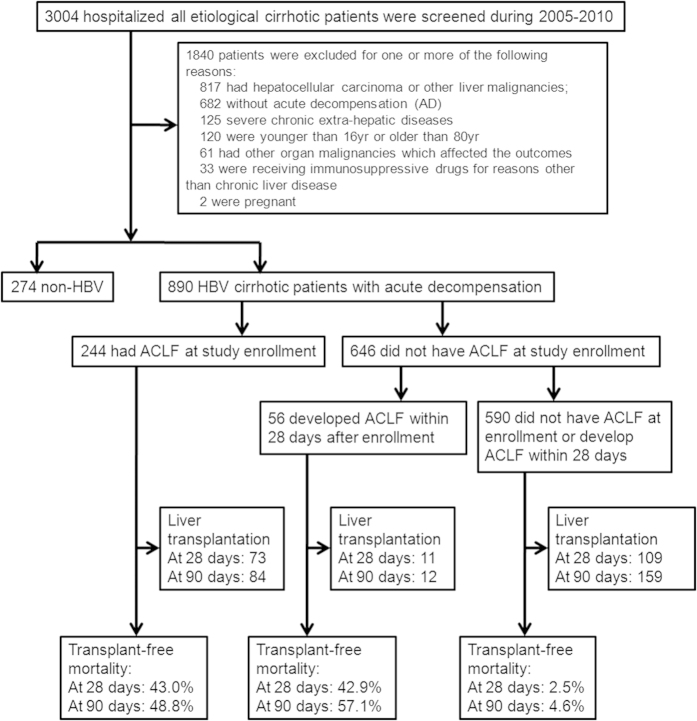
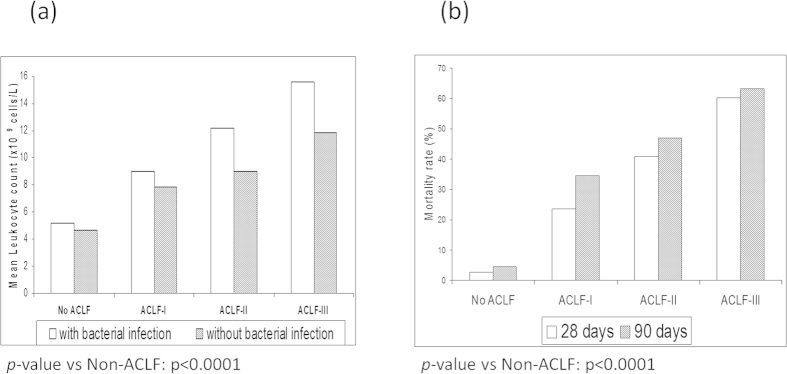
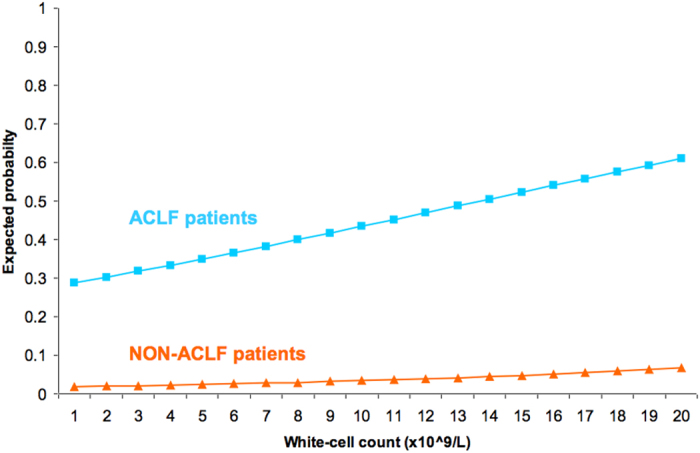
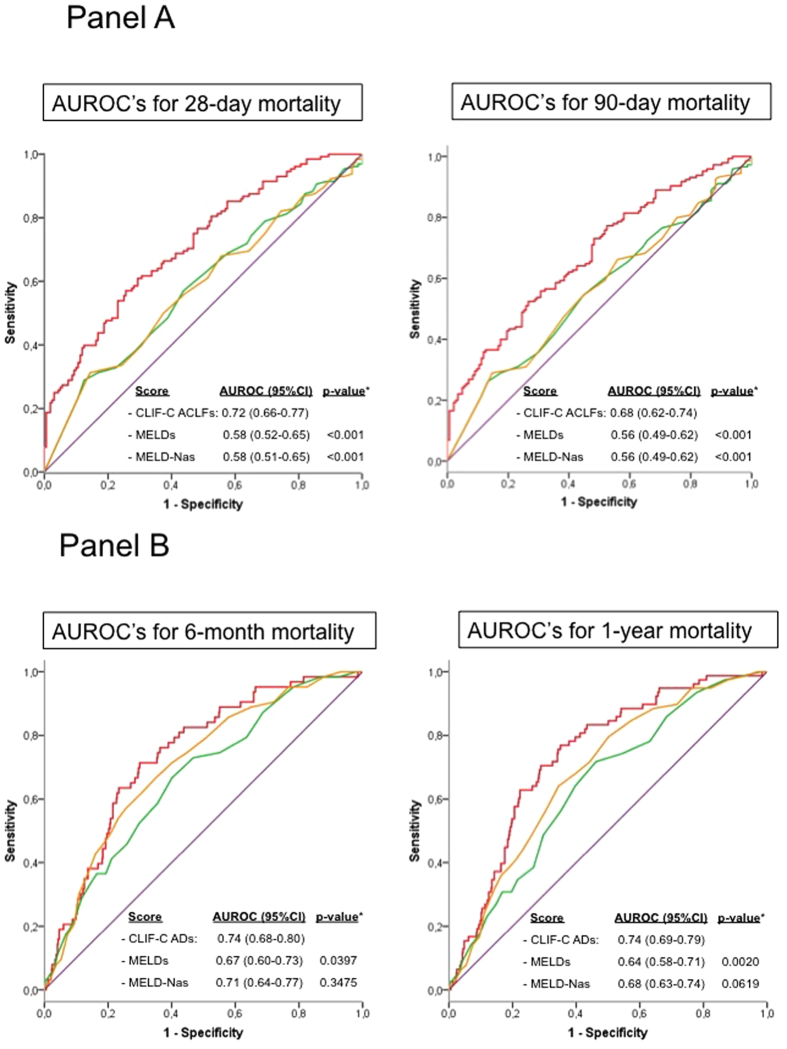
The diagnostic and prognostic criteria of acute-on-chronic liver failure (ACLF) were developed in patients with no Hepatitis B virus (HBV) cirrhosis (CANONIC study). The aims of this study were to evaluate whether the diagnostic (CLIF-C organ failure score; CLIF-C OFs) criteria can be used to classify patients; and the prognostic score (CLIF-C ACLF score) could be used to provide prognostic information in HBV cirrhotic patients with ACLF. 890 HBV associated cirrhotic patients with acute decompensation (AD) were enrolled. Using the CLIF-C OFs, 33.7% (300 patients) were diagnosed as ACLF. ACLF was more common in the younger patients and in those with no previous history of decompensation. The most common organ failures were 'hepatic' and 'coagulation'. As in the CANONIC study, 90-day mortality was extremely low in the non-ACLF patients compared with ACLF patients (4.6% vs 50%, p < 0.0001). ACLF grade and white cell count, were independent predictors of mortality. CLIF-C ACLFs accurately predicted short-term mortality, significantly better than the MELDs and a disease specific score generated for the HBV patients. Current study indicates that ACLF is a clinically and pathophysiology distinct even in HBV patients. Consequently, diagnostic criteria, prognostic scores and probably the management of ACLF should base on similar principles.
Conflict of interest statement
There are potential competing financial interests as follows. Rajiv Jalan received research funding from Vital Therapies, has served on Scientific Advisory Board for Conatus Pharma, and received lecture fees from Gambro and has on-going research collaboration with Gambro, Grifols and is the Principal Investigator of an Industry sponsored study (Sequana Medical). He is also inventor for a drug, L-ornithine phenyl acetate which UCL has licensed to Ocera Therapeutics. Vicente Arroyo has research grants from Grifols.
Figures