

Next-generation sequencing for diagnosis of thoracic aortic aneurysms and dissections: diagnostic yield, novel mutations and genotype phenotype correlations
- PMID: 27146836
- PMCID: PMC4855821
- DOI: 10.1186/s12967-016-0870-4
Next-generation sequencing for diagnosis of thoracic aortic aneurysms and dissections: diagnostic yield, novel mutations and genotype phenotype correlations
Abstract
Background: Thoracic aortic aneurysms and dissections (TAAD) are silent but possibly lethal condition with up to 40 % of cases being hereditary. Genetic background is heterogeneous. Recently next-generation sequencing enabled efficient and cost-effective examination of gene panels. Aim of the study was to define the diagnostic yield of NGS in the 51 TAAD patients and to look for genotype-phenotype correlations within families of the patients with TAAD.
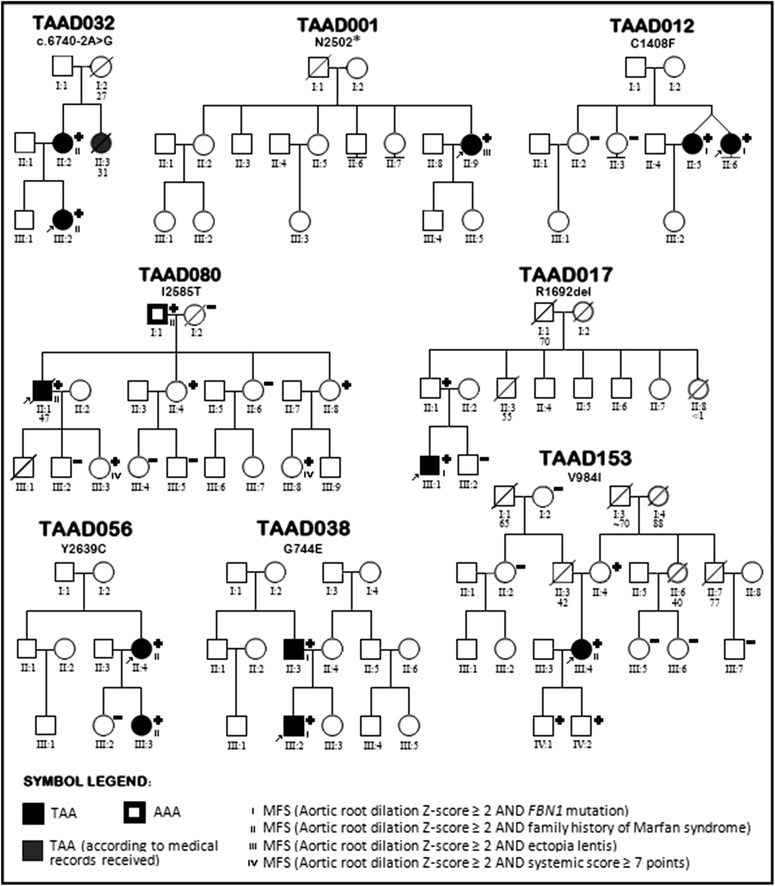
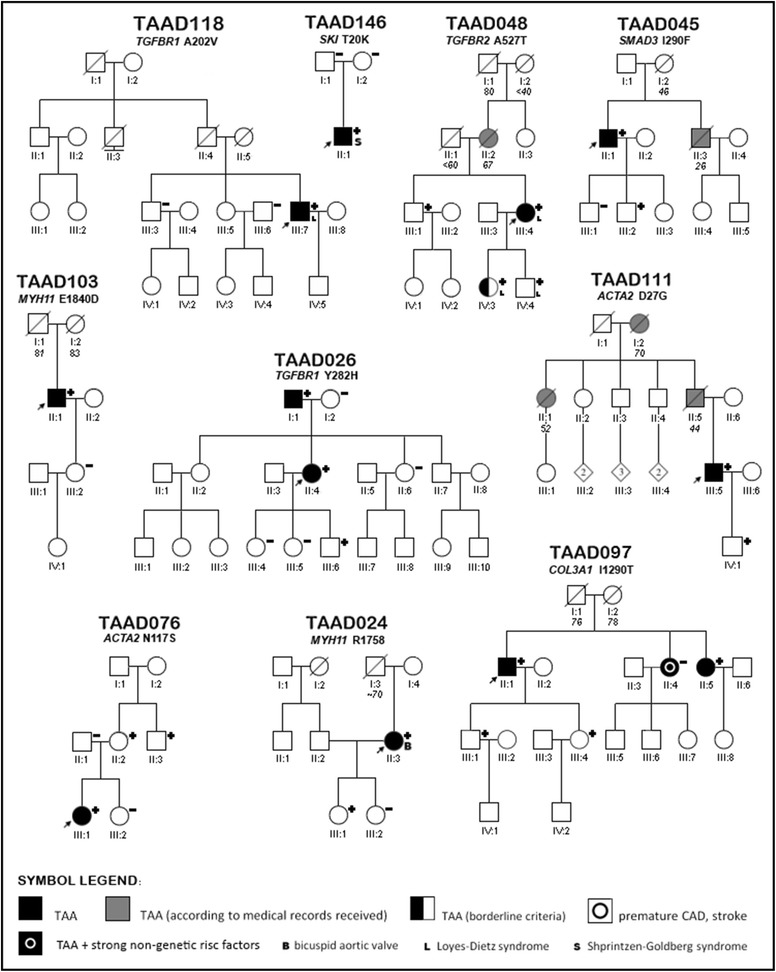
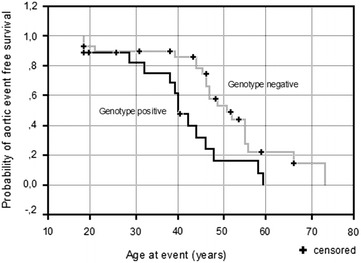
Methods: 51 unrelated TAAD patients were examined by either whole exome sequencing or TruSight One sequencing panel. We analyzed rare variants in 10 established thoracic aortic aneurysms-associated genes. Whenever possible, we looked for co-segregation in the families. Kaplan-Meier survival curve was constructed to compare the event-free survival depending on genotype. Aortic events were defined as acute aortic dissection or first planned aortic surgery.
Results and discussion: In 21 TAAD patients we found 22 rare variants, 6 (27.3 %) of these were previously reported, and 16 (73.7 %) were novel. Based on segregation data, functional analysis and software estimations we assumed that three of novel variants were causative, nine likely causative. Remaining four were classified as of unknown significance (2) and likely benign (2). In all, 9 (17.6 %) of 51 probands had a positive result when considering variants classified as causative only and 18 (35.3 %) if likely causative were also included. Genotype-positive probands (n = 18) showed shorter mean event free survival (41 years, CI 35-46) than reference group, i.e. those (n = 29) without any plausible variant identified (51 years, CI 45-57, p = 0.0083). This effect was also found when the 'genotype-positive' group was restricted to probands with 'likely causative' variants (p = 0.0092) which further supports pathogenicity of these variants. The mean event free survival was particularly low (37 years, CI 27-47) among the probands with defects in the TGF beta signaling (p = 0.0033 vs. the reference group).
Conclusions: This study broadens the spectrum of genetic background of thoracic aneurysms and dissections and supports its potential role as a prognostic factor in the patients with the disease.
Keywords: Diagnosis; Loeys–Dietz syndrome; Marfan syndrome; Next-generation sequencing; Shprintzen–Goldberg syndrome; Thoracic aortic aneurysm and dissections.
Figures
References
-
- Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, Jr, et al. ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121(13):e266–e369. doi: 10.1161/CIR.0b013e3181d4739e. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
