

The Worsening Profile of Alcoholic Hepatitis in the United States
- PMID: 27147285
- PMCID: PMC4918810
- DOI: 10.1111/acer.13069
The Worsening Profile of Alcoholic Hepatitis in the United States
Abstract
Background: Alcoholic hepatitis (AH) is a major cause of liver-related hospitalization. The profile, treatment patterns, and outcomes of subjects admitted for AH in routine clinical practice are unknown. Also, it is not known whether these are changing over time. This study is thus aimed to identify temporal trends in hospitalization rates, clinical characteristics, treatment patterns, and outcomes of subjects admitted for AH in a routine clinical setting.
Methods: A retrospective analysis of adults admitted for AH from 2000 to 2011 was performed using an anonymized EMR database of patient-level data from 169 U.S. medical centers.
Results: (i)
Epidemiology: The proportion of baby boomers admitted for AH increased from 2000 to 2011 (26 to 31%, p < 0.0001). (ii)
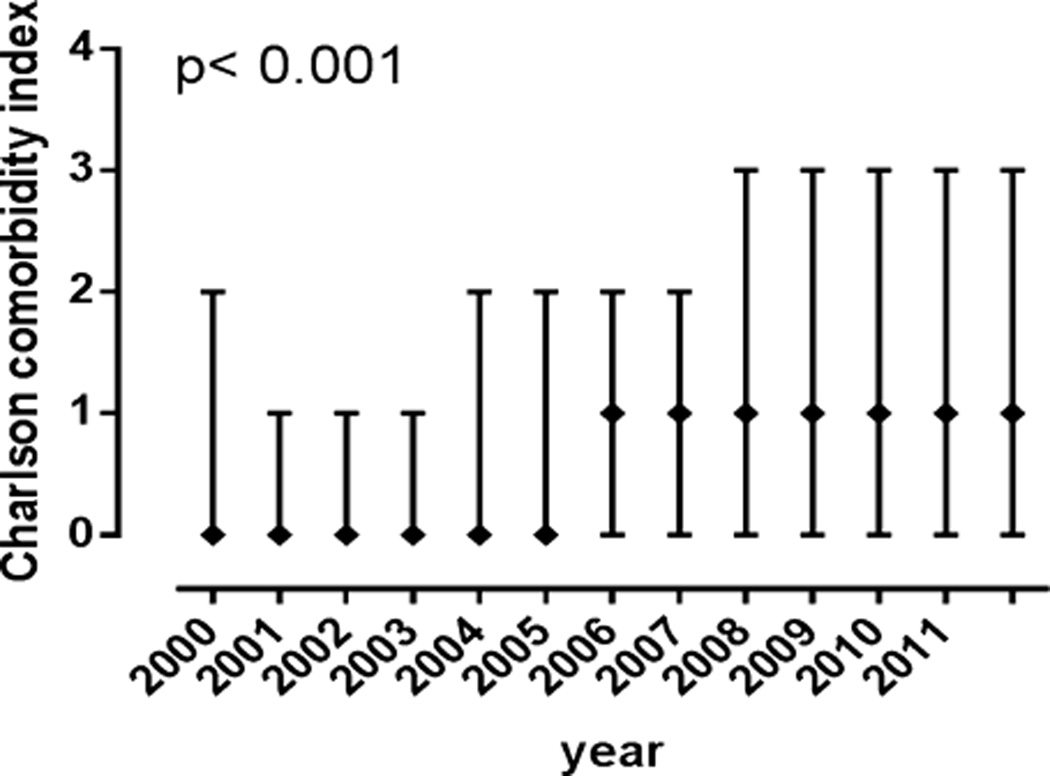
Clinical: The median Model for End-Stage Liver Disease (MELD) score increased over time from 12 to 14 (p = 0.0014) driven mainly by increased international normalized ratio (1.2 to 1.4, p < 0.0001). The median Charlson Comorbidity Index increased from 0 to 1 (p < 0.0001) with increased diabetes, chronic obstructive pulmonary disease, and heart disease. (iii)
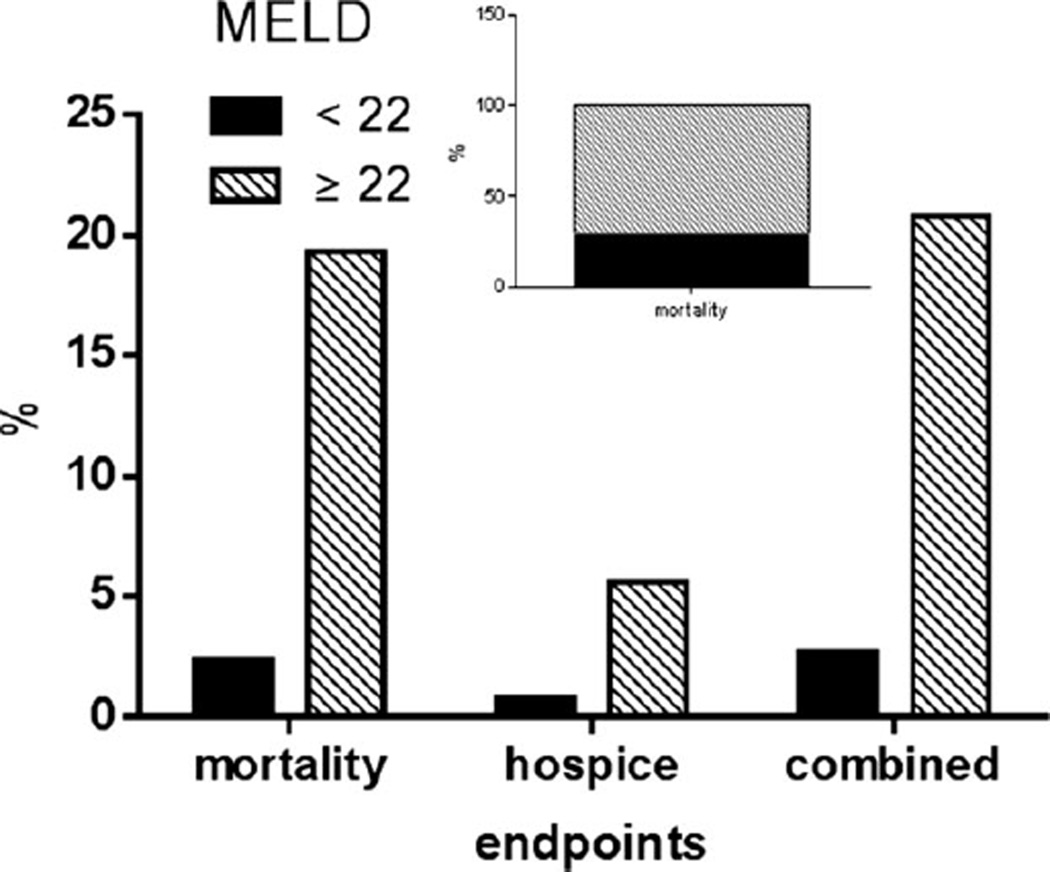
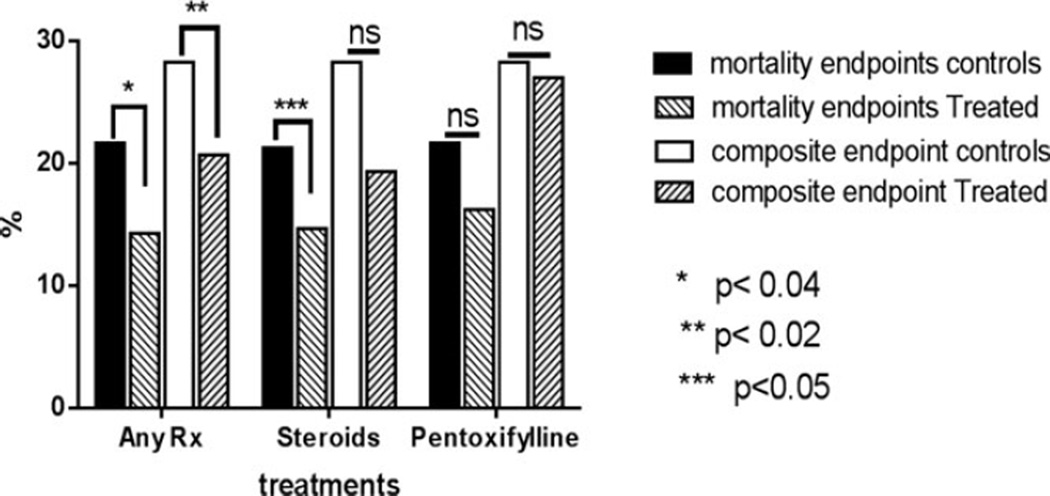
Complications: The following increased from 2001 to 2011: Gastrointestinal bleed-7 to 10% (p = 0.03); hepatic encephalopathy-7 to 13% (p < 0.0001); hepatorenal syndrome-1.8 to 2.8% (p = 0.0003); sepsis-0 to 6% (p < 0.0001); and pancreatitis-11 to 16% (p = 0.0061). (iv) Treatment patterns and mortality: Eight to 9% of subjects received steroids while pentoxifylline use increased to 2.2%. In those with MELD ≥ 22, mortality remained between 19 and 20% and only steroids modestly improved survival in this subset.
Conclusions: Severe AH continues to have a high mortality. The severity and comorbidities and complications associated with AH have worsened. Drug therapy remains suboptimal.
Keywords: Alcohol-Induced Cirrhosis; Alcoholic Hepatitis; Cirrhosis; Lille Score; Liver Failure; Model for End-Stage Liver Disease; Pentoxifylline; Prednisolone; Sepsis; Steroids.
Copyright © 2016 by the Research Society on Alcoholism.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
References
-
- Altamirano J, Miquel R, Katoonizadeh A, Abraldes JG, Duarte-Rojo A, Louvet A, Augustin S, Mookerjee RP, Michelena J, Smyrk TC, Buob D, Leteurtre E, Rincon D, Ruiz P, Garcia-Pagan JC, Guerrero-Marquez C, Jones PD, Barritt AST, Arroyo V, Bruguera M, Banares R, Gines P, Caballeria J, Roskams T, Nevens F, Jalan R, Mathurin P, Shah VH, Bataller R. A histologic scoring system for prognosis of patients with alcoholic hepatitis. Gastroenterology. 2014;146:1231.e6–1239.e1. - PMC - PubMed
-
- Bajaj JS, O’Leary JG, Reddy KR, Wong F, Olson JC, Subramanian RM, Brown G, Noble NA, Thacker LR, Kamath PS, Nacseld Second infections independently increase mortality in hospitalized patients with cirrhosis: the North American consortium for the study of end-stage liver disease (NACSELD) experience. Hepatology. 2012;56:2328–2335. - PMC - PubMed
-
- Casanova J, Bataller R. Alcoholic hepatitis: prognosis and treatment. Gastroenterol Hepatol. 2014;37:262–268. - PubMed
-
- Cortez-Pinto H, Baptista A, Camilo ME, De Moura MC. Nonalcoholic steatohepatitis—a long-term follow-up study: comparison with alcoholic hepatitis in ambulatory and hospitalized patients. Dig Dis Sci. 2003;48:1909–1913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
