

Clinical decision aids for chest pain in the emergency department: identifying low-risk patients
- PMID: 27147894
- PMCID: PMC4806811
- DOI: 10.2147/OAEM.S71282
Clinical decision aids for chest pain in the emergency department: identifying low-risk patients
Abstract
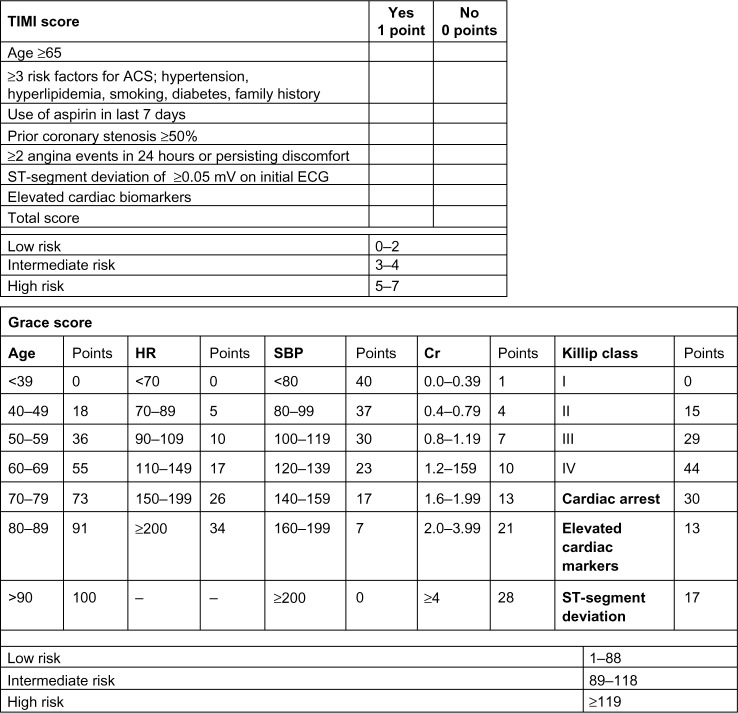
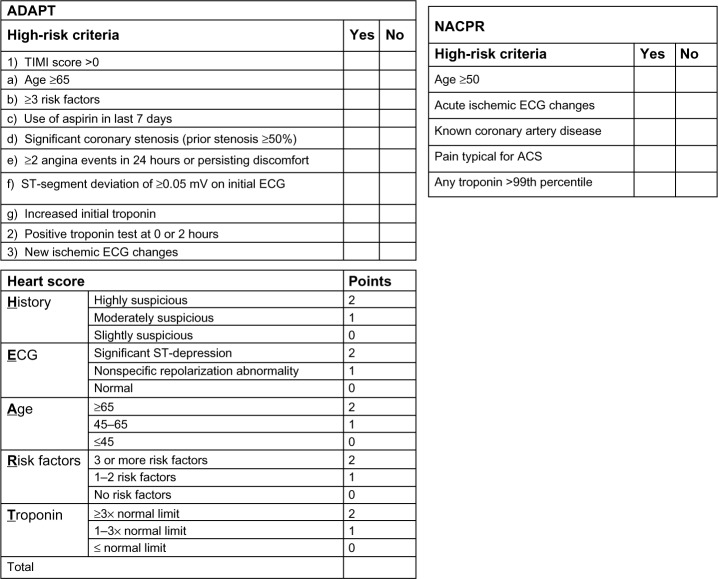
Chest pain is one of the most common presenting complaints in the emergency department, though only a small minority of patients are subsequently diagnosed with acute coronary syndrome (ACS). However, missing the diagnosis has potential for significant morbidity and mortality. ACS presentations can be atypical, and their workups are often prolonged and costly. In order to risk-stratify patients and better direct the workup and care given, many decision aids have been developed. While each may have merit in certain clinical settings, the most useful aid in the emergency department is one that finds all cases of ACS while also identifying a substantial subset of patients at low risk who can be discharged without stress testing or coronary angiography. This review describes several of the chest pain decision aids developed and studied through the recent past, starting with the thrombolysis in myocardial infarction (TIMI) risk score and Global Registry of Acute Coronary Events (GRACE) scores, which were developed as prognostic aids for patients already diagnosed with ACS, then subsequently validated in the undifferentiated chest pain population. Asia-Pacific Evaluation of Chest Pain Trial (ASPECT); Accelerated Diagnostic Protocol to Assess Patients With Chest Pain Symptoms Using Contemporary Troponins (ADAPT); North American Chest Pain Rule (NACPR); and History, Electrocardiogram, Age, Risk factors, Troponin (HEART) score have been developed exclusively for use in the undifferentiated chest pain population as well, with improved performance compared to their predecessors. This review describes the relative merits and limitations of these decision aids so that providers can determine which tool fits the needs of their clinical practice setting.
Keywords: acute coronary syndrome; chest pain; decision aid; risk score.
Figures
Similar articles
-
Comparison of nine coronary risk scores in evaluating patients presenting to hospital with undifferentiated chest pain.Int J Gen Med. 2018 Dec 13;11:473-481. doi: 10.2147/IJGM.S183583. eCollection 2018. Int J Gen Med. 2018. PMID: 30588062 Free PMC article.
-
Validation of high-sensitivity troponin I in a 2-hour diagnostic strategy to assess 30-day outcomes in emergency department patients with possible acute coronary syndrome.J Am Coll Cardiol. 2013 Oct 1;62(14):1242-1249. doi: 10.1016/j.jacc.2013.02.078. Epub 2013 Apr 10. J Am Coll Cardiol. 2013. PMID: 23583250 Clinical Trial.
-
Prognosticating Clinical Prediction Scores Without Clinical Gestalt for Patients With Chest Pain in the Emergency Department.J Emerg Med. 2018 Feb;54(2):176-185. doi: 10.1016/j.jemermed.2017.10.006. Epub 2017 Nov 27. J Emerg Med. 2018. PMID: 29191490
-
[Is a more efficient operative strategy feasible for the emergency management of the patient with acute chest pain?].Ital Heart J Suppl. 2000 Feb;1(2):186-201. Ital Heart J Suppl. 2000. PMID: 10731376 Review. Italian.
-
Best Clinical Practice: Current Controversies in Evaluation of Low-Risk Chest Pain-Part 1.J Emerg Med. 2016 Dec;51(6):668-676. doi: 10.1016/j.jemermed.2016.07.103. Epub 2016 Sep 29. J Emerg Med. 2016. PMID: 27693075 Review.
Cited by
-
Lethal means counseling for suicide prevention: Views of emergency department clinicians.Gen Hosp Psychiatry. 2021 Jul-Aug;71:95-101. doi: 10.1016/j.genhosppsych.2021.04.011. Epub 2021 May 6. Gen Hosp Psychiatry. 2021. PMID: 33971519 Free PMC article.
-
Predictive risk stratification using HEART (history, electrocardiogram, age, risk factors, and initial troponin) and TIMI (thrombolysis in myocardial infarction) scores in non-high risk chest pain patients: An African American urban community based hospital study.Medicine (Baltimore). 2019 Aug;98(32):e16370. doi: 10.1097/MD.0000000000016370. Medicine (Baltimore). 2019. PMID: 31393346 Free PMC article.
-
Acute chest pain after bench press exercise in a healthy young adult.Open Access Emerg Med. 2016 Sep 22;8:73-76. doi: 10.2147/OAEM.S114310. eCollection 2016. Open Access Emerg Med. 2016. PMID: 27703399 Free PMC article.
-
Comparison of nine coronary risk scores in evaluating patients presenting to hospital with undifferentiated chest pain.Int J Gen Med. 2018 Dec 13;11:473-481. doi: 10.2147/IJGM.S183583. eCollection 2018. Int J Gen Med. 2018. PMID: 30588062 Free PMC article.
-
Yangxin Decoction combined acupuncture on blood lipid metabolism in Qi Deficiency and Blood Stasis type of Chest Bi-Syndrome: A protocol of systematic review.Medicine (Baltimore). 2020 Aug 21;99(34):e21744. doi: 10.1097/MD.0000000000021744. Medicine (Baltimore). 2020. PMID: 32846797 Free PMC article.
References
-
- Bhuiya FA, Pitts SR, McCaig LF. Emergency department visits for chest pain and abdominal pain: United States, 1999–2008. NCHS Data Brief. 2010;(43):1–8. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342(16):1163–1170. - PubMed
-
- Than M, Herbert M, Flaws D, et al. What is an acceptable risk of major adverse cardiac event in chest pain patients soon after discharge from the Emergency Department? A clinical survey. Int J Cardiol. 2013;166(3):752–754. - PubMed
-
- Antman EM, Cohen M, Bernink PM, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284(7):835–842. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
