

Comparison of the Bedside Head-Impulse Test with the Video Head-Impulse Test in a Clinical Practice Setting: A Prospective Study of 500 Outpatients
- PMID: 27148159
- PMCID: PMC4837142
- DOI: 10.3389/fneur.2016.00058
Comparison of the Bedside Head-Impulse Test with the Video Head-Impulse Test in a Clinical Practice Setting: A Prospective Study of 500 Outpatients
Abstract
Objectives: The primary aim was to determine the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the bedside head-impulse test (bHIT) using the video HIT (vHIT) as the gold standard for quantifying the function of the vestibulo-ocular reflex (VOR). Secondary aims were to determine the bHIT inter-rater reliability and sensitivity in detecting unilateral and bilateral vestibulopathy.
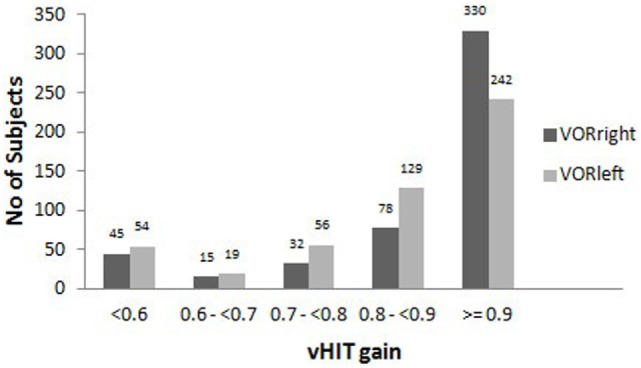
Methods: In this prospective study, 500 consecutive outpatients presenting to a tertiary neuro-otology clinic with vertigo or dizziness of various vestibular etiologies who did not have any of the pre-defined exclusion criteria were recruited. Bedside HITs were done by three experienced neuro-otology clinicians masked to the diagnosis, and the results were compared with the vHIT. The patients were likewise blinded to the bHIT and vHIT findings. Patients with VOR deficits were identified on the vHIT by referencing to the pre-selected "pathological" gain of <0.7. The data were then analyzed using standard statistical methods.
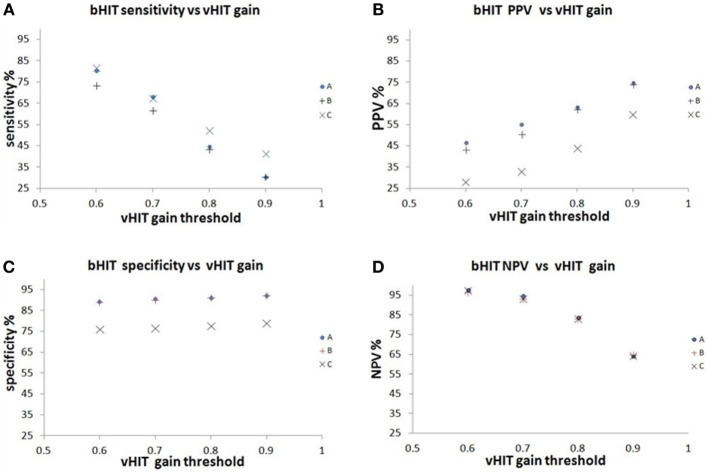
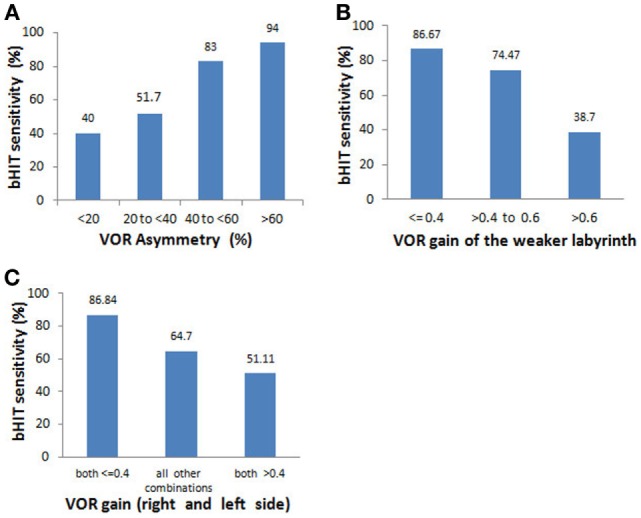
Results: For the primary outcome (vHIT "pathological" VOR gain <0.7), the three-rater mean bHIT sensitivity = 66.0%, PPV = 44.3%, specificity = 86.2%, and NPV = 93.9%. Shifting the "pathological" threshold from 0.6 to 0.9 caused the bHIT sensitivity to decrease while the PPV increased. Specificity and NPV tended to remain stable. Inter-rater agreement was moderate (Krippendorff's alpha = 0.54). For unilateral vestibulopathy, overall bHIT sensitivity = 69.6%, reaching 86.67% for severely reduced unilateral gain. For VOR asymmetry <40% and >40%, the bHIT sensitivity = 51.7 and 83%, respectively. For bilateral vestibulopathy, overall bHIT sensitivity = 66.3%, reaching 86.84% for severely reduced bidirectional gains.
Conclusion: For the primary outcome, the bHIT had moderate sensitivity and low PPV. While the study did not elucidate the best choice for vHIT reference, it demonstrated how the bHIT test properties varied with vHIT thresholds: selecting a lower threshold improved the sensitivity but diminished the PPV, while a higher threshold had the opposite effect. The VOR was most likely normal if the bHIT was negative due to its high NPV. The bHIT was moderately sensitive for detecting unilateral and bilateral vestibulopathy overall, but better for certain subgroups.
Keywords: head-impulse test; negative predictive value; positive predictive value; sensitivity; specificity; vestibulo-ocular reflex.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources