

Tertiary Lymphoid Organs in Takayasu Arteritis
- PMID: 27148274
- PMCID: PMC4840206
- DOI: 10.3389/fimmu.2016.00158
Tertiary Lymphoid Organs in Takayasu Arteritis
Abstract
Objective: The role of B cells in the pathogenesis of Takayasu arteritis (TA) is controversial. We aimed to study the presence of tertiary lymphoid organs (TLOs) in the aortic wall of TA patients.
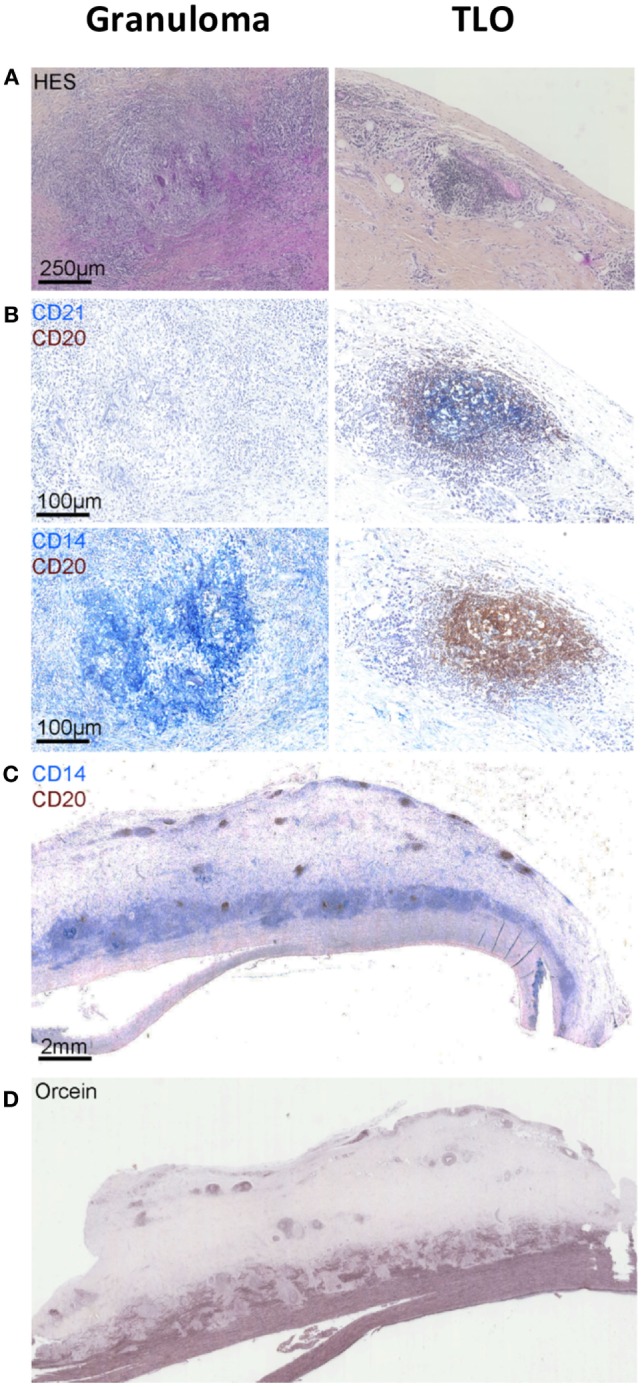
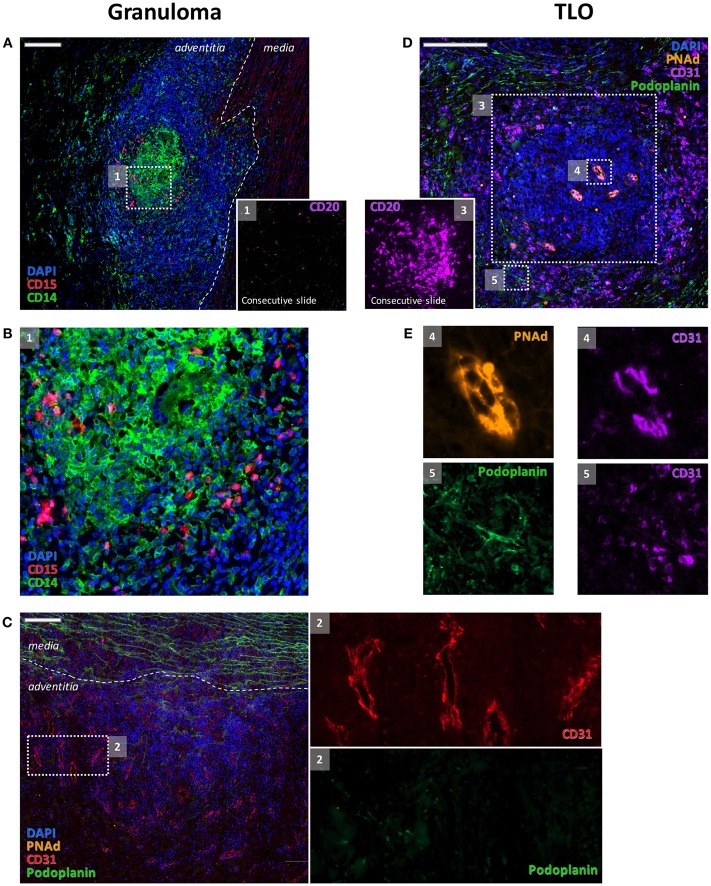
Methods: Hematoxylin and eosin-stained sections from aorta specimens from patients with TA were screened for TLOs. The presence of B cell aggregates (CD20), follicular dendritic cells (FDCs, CD21), and high endothelial venules (HEVs, PNAd) was investigated by immunohistochemistry. Immune cells from the adventitial layer of one patient were characterized by flow cytometry. Demographic, medical history, laboratory, imaging, treatment, and follow-up data were extracted from medical records.
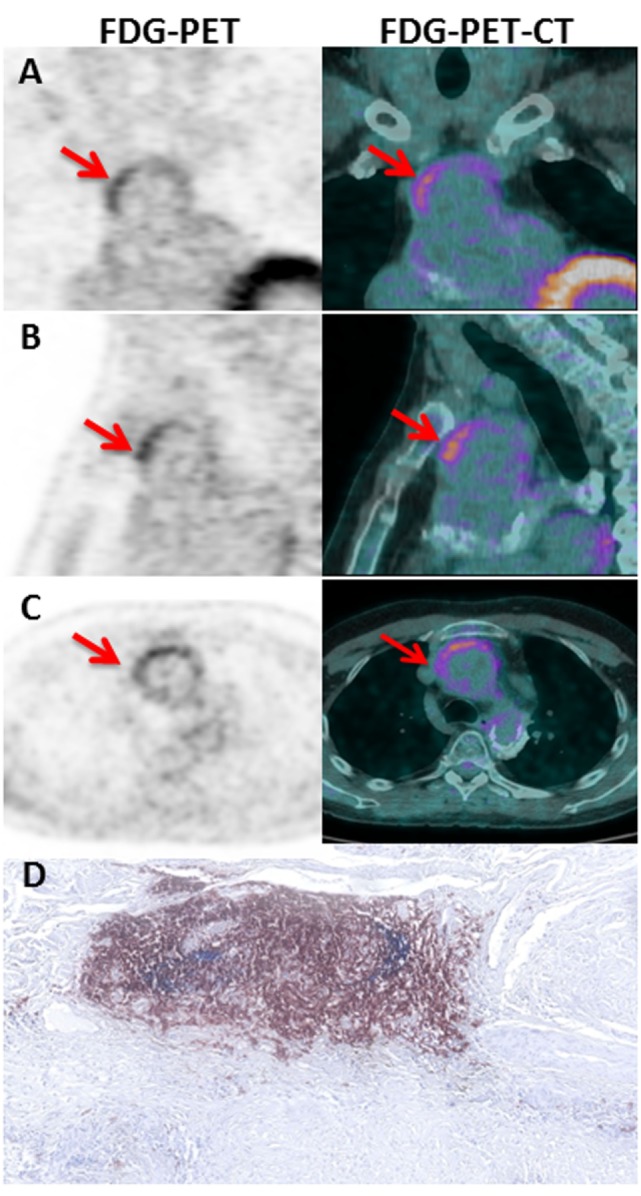
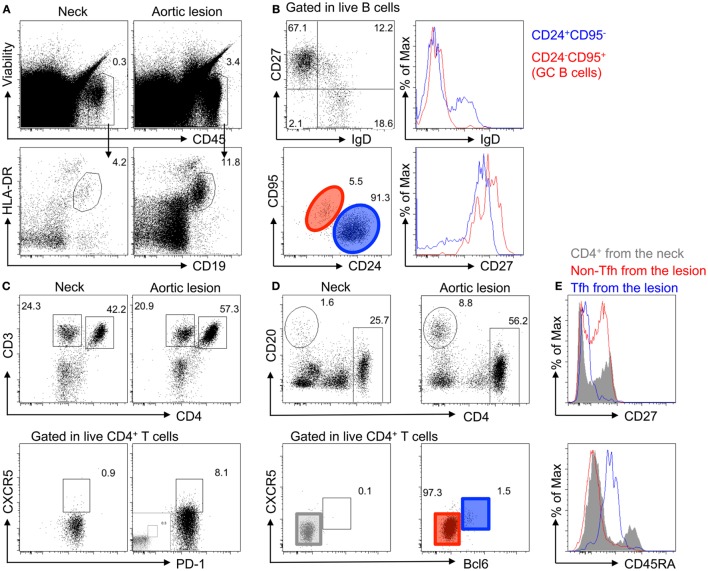
Results: Aorta specimens from Bentall procedures were available from seven patients (5 females, aged 22-57 years) with TA. Surgical treatment was performed at TA diagnosis (n = 4) or at a median of 108 months (84-156) after TA diagnosis. Disease was active at surgery in four patients according to NIH score. B cell aggregates-TLOs containing HEVs were observed in the adventitia of all but one patient. Of note, ectopic follicles containing CD21(+) FDCs were found in all patients (4/4) with increased aortic (18)F-fluoro-deoxyglucose (FDG) uptake before surgery but were absent in all but one patients (2/3) with no FDG uptake. In addition, flow cytometry analysis confirmed the accumulation of memory/germinal center-like B cells in the adventitial layer and showed the presence of antigen-experienced T follicular helper cells.
Conclusion: Ectopic lymphoid neogenesis displaying functional features can be found in the aortic wall of a subset of patients with active TA. The function of these local B cell clusters on the pathogenesis of TA remains to be elucidated.
Keywords: B cells; Takayasu arteritis; immunopathogenesis; tertiary lymphoid organs.
Figures
References
-
- Clement M, Guedj K, Andreata F, Morvan M, Bey L, Khallou-Laschet J, et al. Control of the T follicular helper-germinal center B-cell axis by CD8(+) regulatory T cells limits atherosclerosis and tertiary lymphoid organ development. Circulation (2015) 131:560–70. 10.1161/CIRCULATIONAHA.114.010988 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources