

Enhanced Recovery After Surgery Program in Patients Undergoing Pancreaticoduodenectomy: A PRISMA-Compliant Systematic Review and Meta-Analysis
- PMID: 27149448
- PMCID: PMC4863765
- DOI: 10.1097/MD.0000000000003497
Enhanced Recovery After Surgery Program in Patients Undergoing Pancreaticoduodenectomy: A PRISMA-Compliant Systematic Review and Meta-Analysis
Abstract
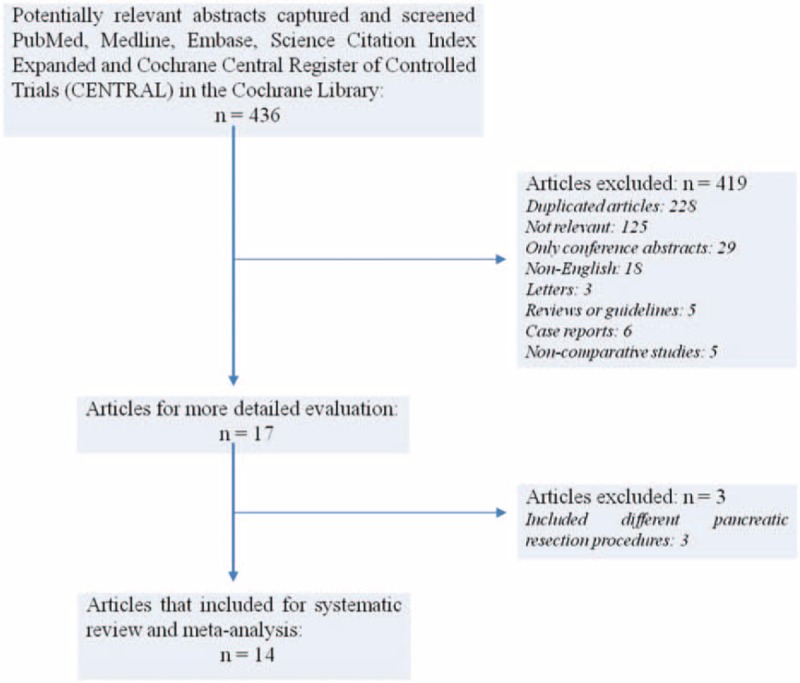
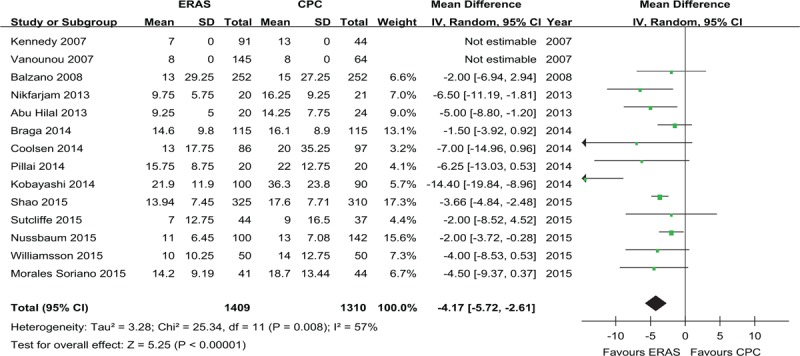
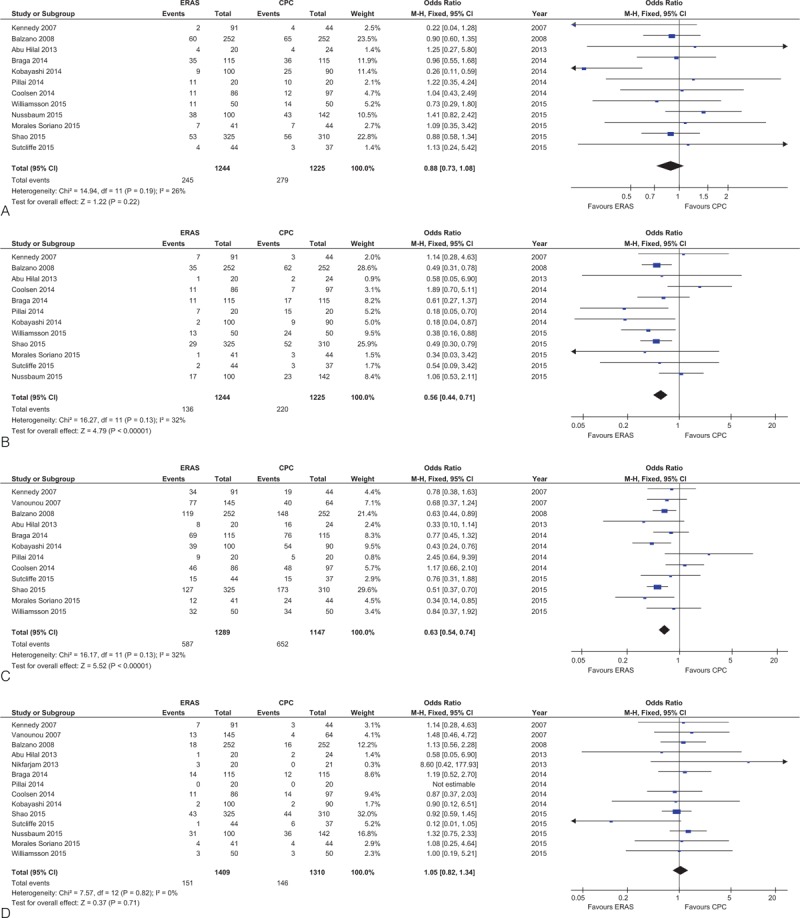
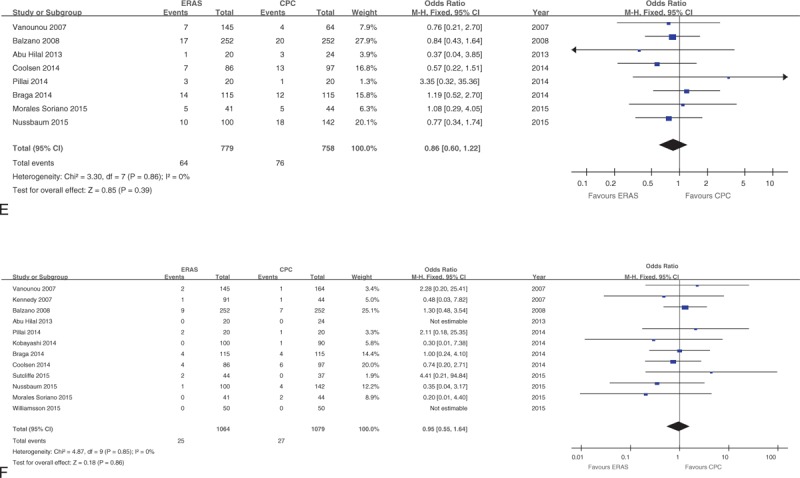
Enhanced recovery after surgery (ERAS) pathways are multimodal, evidence-based approaches to optimize patient outcome after surgery. However, the use of ERAS protocols to improve morbidity and recovery time without compromising safety following pancreaticoduodenectomy (PD) remains to be elucidated.We conducted a systemic review and meta-analysis to assess the safety and efficacy of ERAS protocols compared with conventional perioperative care (CPC) in patients following PD.PubMed, Medline, Embase, and Science Citation Index Expanded and Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library were searched between January 2000 and June 2015.The patients who underwent PD with ERAS protocols or CPC were eligible. The studies that compared postoperative length of hospital stay (PLOS), postoperative complications, or in-hospital costs in the 2 groups were included.A meta-analysis, meta-regression, sensitivity analysis, and subgroup analysis were performed to estimate the postoperative outcomes between the 2 groups and identified the potential confounders. We used the methodological index for nonrandomized studies checklist to assess methodological qualities. Weighted mean differences (WMD) or odds ratios (OR) were calculated with their corresponding 95% confidence intervals (CI). The publication bias tests were also performed through the funnel plots.In total, 14 nonrandomized comparative studies with 1409 ERAS cases and 1310 controls were analyzed. Implementation of an ERAS protocol significantly reduced PLOS (WMD: -4.17 days; 95%CI: -5.72 to -2.61), delayed gastric emptying (OR: 0.56; 95%CI: 0.44-0.71), overall morbidity (OR: 0.63; 95% CI: 0.54-0.74), and in-hospital costs compared to CPC (all P < 0.001). There were no statistically significant differences in other postoperative outcomes. Age, gender, and ERAS component implementation did not significantly contribute to heterogeneity for PLOS as shown by meta-regression analysis.Our study suggested that ERAS was as safe as CPC and improved recovery of patients undergoing PD, thus reducing in-hospital costs. General adoption of ERAS protocols during PD should be recommended.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002; 183:630–641. - PubMed
-
- Fearon KC, Ljungqvist O, Von Meyenfeldt M, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005; 24:466–477. - PubMed
-
- Weber WP, Barry M, Junqueira MJ, et al. Initial experiences with a multidisciplinary approach to decreasing the length of hospital stay for patients undergoing unilateral mastectomy. EJSO 2011; 37:944–949. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
