

Gait kinematics and kinetics are affected more by peripheral arterial disease than by age
- PMID: 27149635
- PMCID: PMC4898204
- DOI: 10.1682/JRRD.2015.02.0027
Gait kinematics and kinetics are affected more by peripheral arterial disease than by age
Abstract
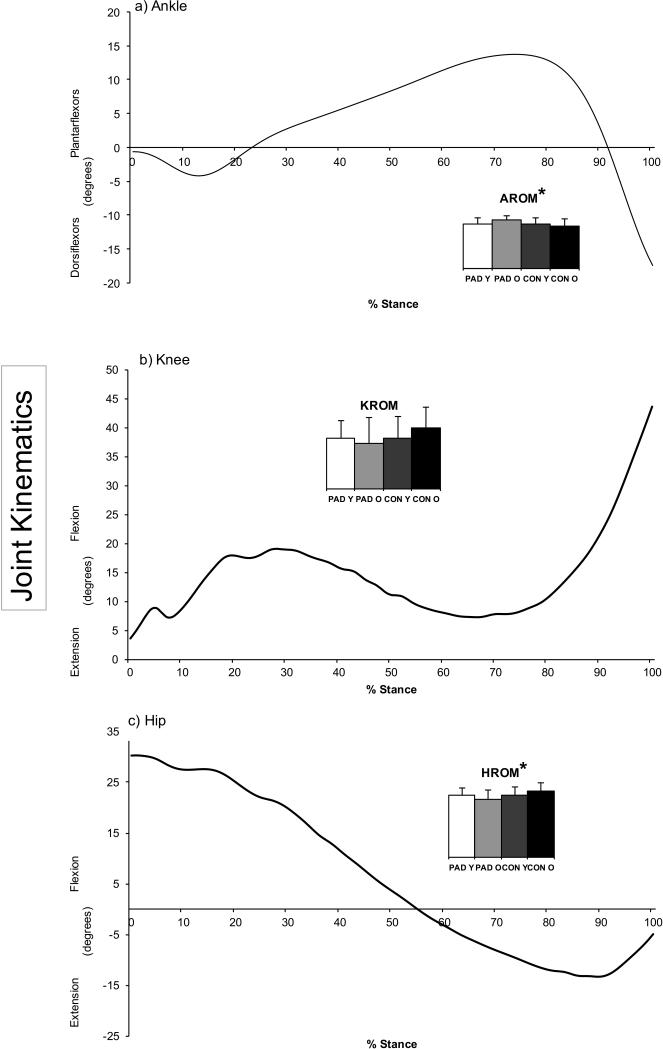
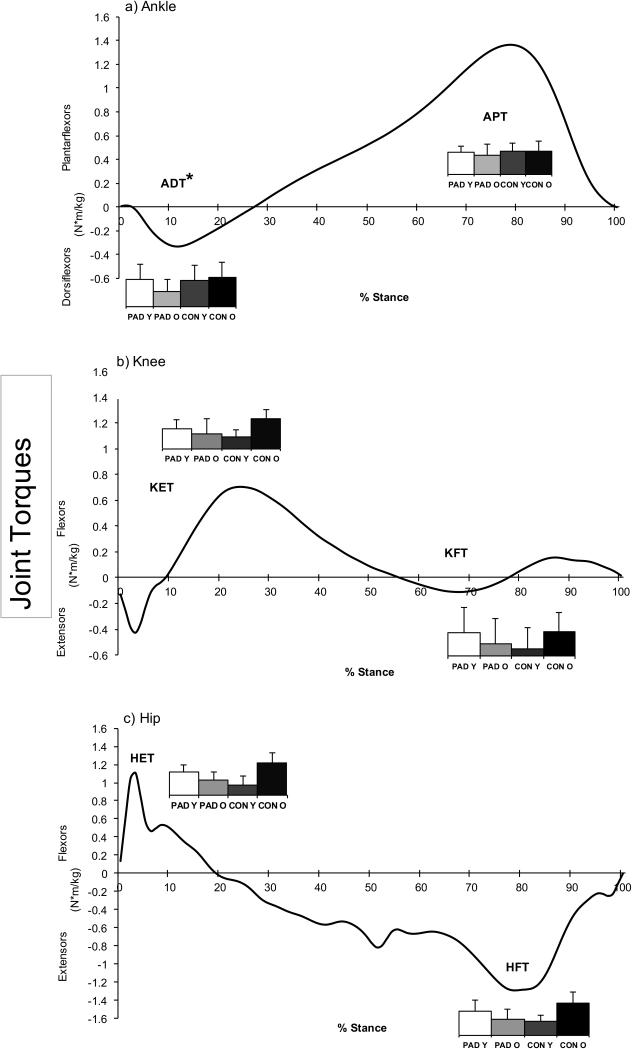
Peripheral arterial disease (PAD) produces abnormal gait and disproportionately affects older individuals. The current study investigated PAD gait biomechanics in younger (<65 yr) and older (>/=65 yr) subjects. The study included 61 patients with PAD (31 younger, age: 57.4 +/- 5.3 yr, and 30 older, age: 71.9 +/- 5.2 yr) and 52 nondisabled age-matched control subjects. Patients with PAD were tested during pain-free walking and compared with control subjects. Joint kinematics and kinetics (torques) were compared using a 2 x 2 analysis of variance (groups: patients with PAD vs control subjects, age: younger vs older). Patients with PAD had significantly increased ankle and decreased hip range of motion during the stance phase as well as decreased ankle dorsiflexor torque compared with control subjects. Gait changes in older individuals are largely constrained to time-distance parameters. Joint kinematics and kinetics are significantly altered in patients with PAD during pain-free walking. Symptomatic PAD produces a consistent ambulatory deficit across ages definable by advanced biomechanical analysis. The most important finding of the current study is that gait, in the absence of PAD and other ambulatory comorbidities, does not decline significantly with age based on advanced biomechanical analysis. Therefore, previous studies must be examined in the context of patients with potential PAD being present in the population, and future ambulatory studies must include PAD as a confounding factor when assessing the gait function of elderly individuals.
Trial registration: ClinicalTrials.gov NCT00094575.
Keywords: aging; biomechanics; gait; gait decline; joint angles; joint torques; older adults; peripheral arterial disease; peripheral vascular disease; walking.
Figures
Similar articles
-
A biomechanical perspective on walking in patients with peripheral artery disease.Vasc Med. 2023 Feb;28(1):77-84. doi: 10.1177/1358863X221146207. Vasc Med. 2023. PMID: 36759931 Free PMC article. Review.
-
Peripheral arterial disease affects kinematics during walking.J Vasc Surg. 2009 Jan;49(1):127-32. doi: 10.1016/j.jvs.2008.08.013. Epub 2008 Nov 22. J Vasc Surg. 2009. PMID: 19028062
-
Joint torques and powers are reduced during ambulation for both limbs in patients with unilateral claudication.J Vasc Surg. 2010 Jan;51(1):80-8. doi: 10.1016/j.jvs.2009.07.117. Epub 2009 Oct 17. J Vasc Surg. 2010. PMID: 19837536 Free PMC article.
-
Relationship between temporal-spatial gait parameters, gait kinematics, walking performance, exercise capacity, and physical activity level in peripheral arterial disease.J Vasc Surg. 2007 Jun;45(6):1172-8. doi: 10.1016/j.jvs.2007.01.060. J Vasc Surg. 2007. PMID: 17543681
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
Cited by
-
Changes in Gait Variables in Patients with Intermittent Claudication.Biomed Res Int. 2019 May 27;2019:7276865. doi: 10.1155/2019/7276865. eCollection 2019. Biomed Res Int. 2019. PMID: 31263707 Free PMC article.
-
Relationship Between Physical Performance and Peripheral Arterial Diseases in Different Age Groups of Chinese Community-Dwelling Older Adults.J Atheroscler Thromb. 2023 Jul 1;30(7):778-785. doi: 10.5551/jat.63697. Epub 2022 Oct 1. J Atheroscler Thromb. 2023. PMID: 36184558 Free PMC article.
-
Impaired microcirculatory function, mitochondrial respiration, and oxygen utilization in skeletal muscle of claudicating patients with peripheral artery disease.Am J Physiol Heart Circ Physiol. 2022 May 1;322(5):H867-H879. doi: 10.1152/ajpheart.00690.2021. Epub 2022 Mar 25. Am J Physiol Heart Circ Physiol. 2022. PMID: 35333113 Free PMC article.
-
A biomechanical perspective on walking in patients with peripheral artery disease.Vasc Med. 2023 Feb;28(1):77-84. doi: 10.1177/1358863X221146207. Vasc Med. 2023. PMID: 36759931 Free PMC article. Review.
-
Characteristics of Plantar Pressure Distribution in Diabetes with or without Diabetic Peripheral Neuropathy and Peripheral Arterial Disease.J Healthc Eng. 2022 Jun 6;2022:2437831. doi: 10.1155/2022/2437831. eCollection 2022. J Healthc Eng. 2022. PMID: 35707567 Free PMC article.
References
-
- Nehler MR, McDermott MM, Treat-Jacobson D, Chetter I, Regensteiner JG. Functional outcomes and quality of life in peripheral arterial disease: current status. VASC MED. 2003;8(2):115–26. - PubMed
-
- Nicoloff AD, Taylor LM, Jr., McLafferty RB, Moneta GL, Porter JM. Patient recovery after infrainguinal bypass grafting for limb salvage. J Vasc Surg. 1998;27(2):256–63. discussion 64-6. - PubMed
-
- Toursarkissian B, Shireman PK, Harrison A, D'Ayala M, Schoolfield J, Sykes MT. Major lower-extremity amputation: contemporary experience in a single Veterans Affairs institution. The American surgeon. 2002;68(7):606–10. - PubMed
-
- Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, Hiatt WR. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical