

Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review
- PMID: 27152255
- PMCID: PMC4848155
- DOI: 10.5492/wjccm.v5.i2.121
Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review
Abstract
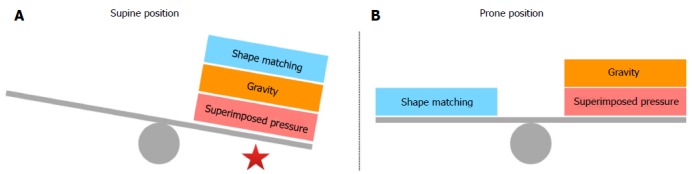
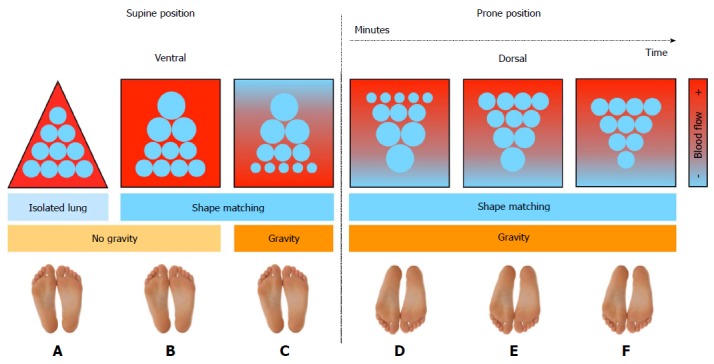
Acute respiratory distress syndrome (ARDS) is a syndrome with heterogeneous underlying pathological processes. It represents a common clinical problem in intensive care unit patients and it is characterized by high mortality. The mainstay of treatment for ARDS is lung protective ventilation with low tidal volumes and positive end-expiratory pressure sufficient for alveolar recruitment. Prone positioning is a supplementary strategy available in managing patients with ARDS. It was first described 40 years ago and it proves to be in alignment with two major ARDS pathophysiological lung models; the "sponge lung" - and the "shape matching" -model. Current evidence strongly supports that prone positioning has beneficial effects on gas exchange, respiratory mechanics, lung protection and hemodynamics as it redistributes transpulmonary pressure, stress and strain throughout the lung and unloads the right ventricle. The factors that individually influence the time course of alveolar recruitment and the improvement in oxygenation during prone positioning have not been well characterized. Although patients' response to prone positioning is quite variable and hard to predict, large randomized trials and recent meta-analyses show that prone position in conjunction with a lung-protective strategy, when performed early and in sufficient duration, may improve survival in patients with ARDS. This pathophysiology-based review and recent clinical evidence strongly support the use of prone positioning in the early management of severe ARDS systematically and not as a rescue maneuver or a last-ditch effort.
Keywords: Acute respiratory distress syndrome; Mechanical ventilation; Pathophysiology; Prone position; Ventilator-induced lung injury.
Figures

References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2:319–323. - PubMed
-
- Linko R, Okkonen M, Pettilä V, Perttilä J, Parviainen I, Ruokonen E, Tenhunen J, Ala-Kokko T, Varpula T. Acute respiratory failure in intensive care units. FINNALI: a prospective cohort study. Intensive Care Med. 2009;35:1352–1361. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
