

Cost effectiveness of intensive care in a low resource setting: A prospective cohort of medical critically ill patients
- PMID: 27152258
- PMCID: PMC4848158
- DOI: 10.5492/wjccm.v5.i2.150
Cost effectiveness of intensive care in a low resource setting: A prospective cohort of medical critically ill patients
Abstract
Aim: To calculate cost effectiveness of the treatment of critically ill patients in a medical intensive care unit (ICU) of a middle income country with limited access to ICU resources.
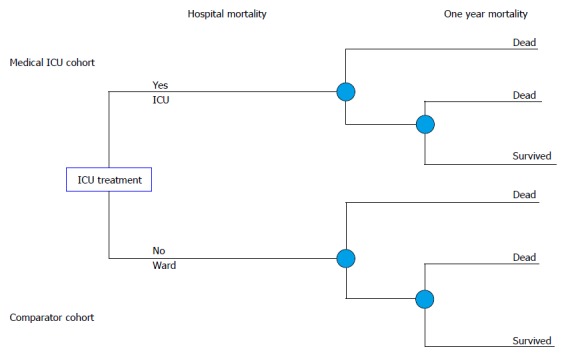
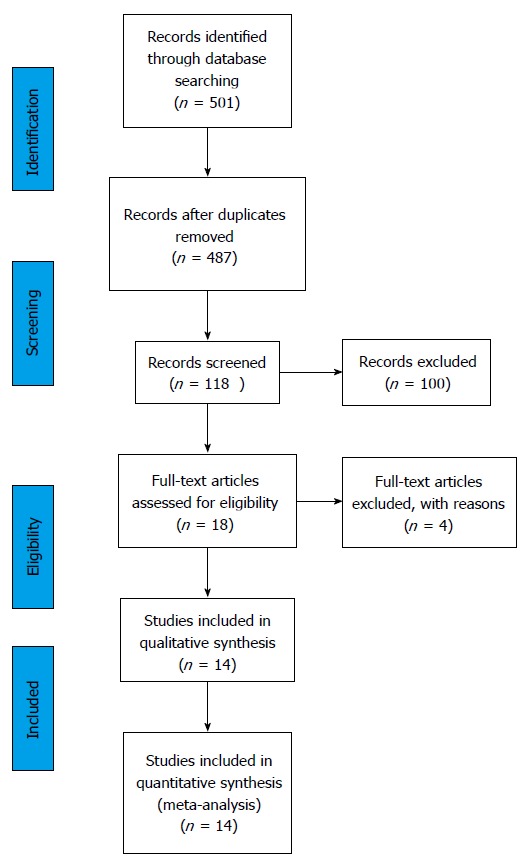
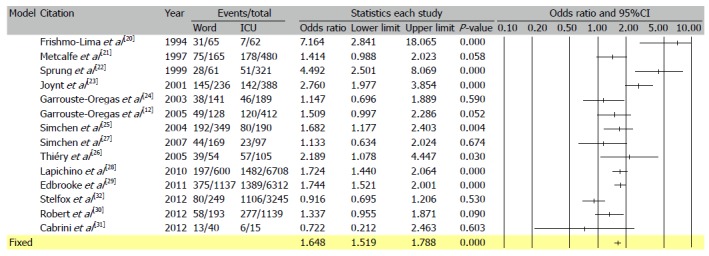
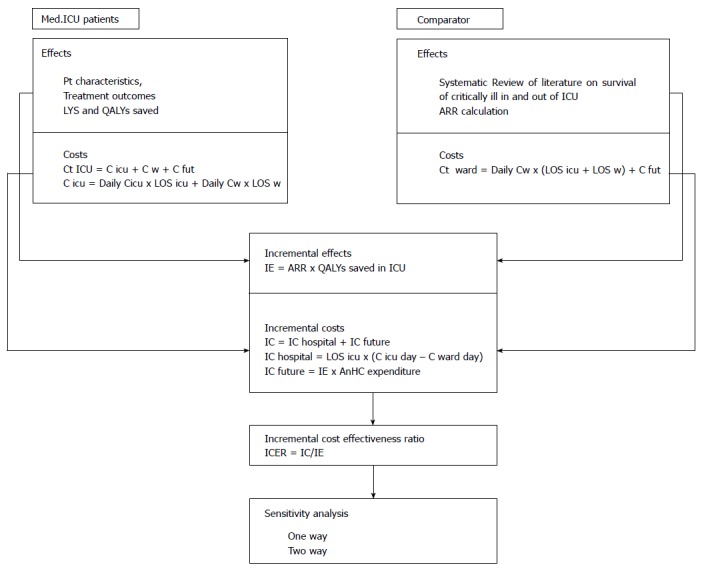
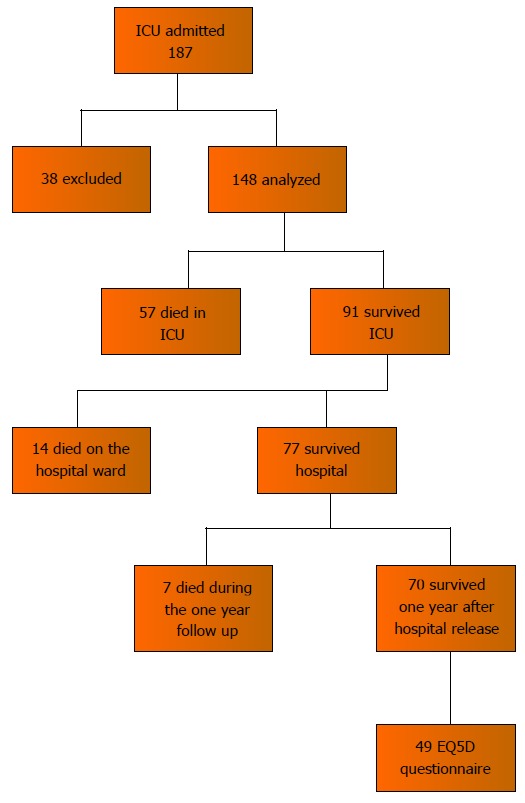
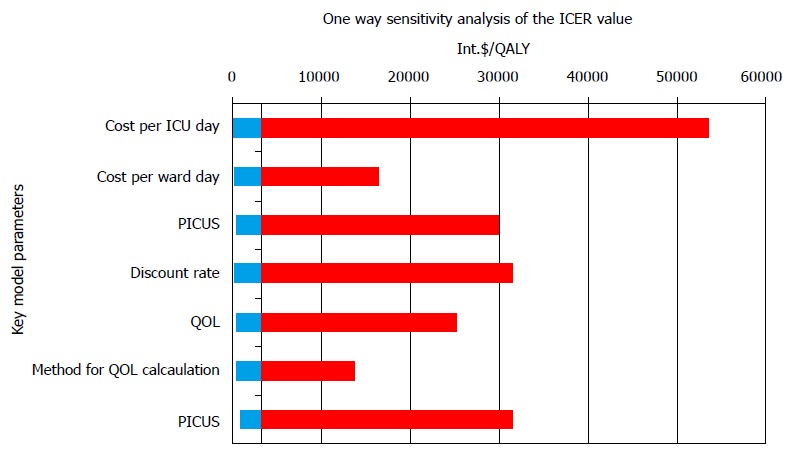
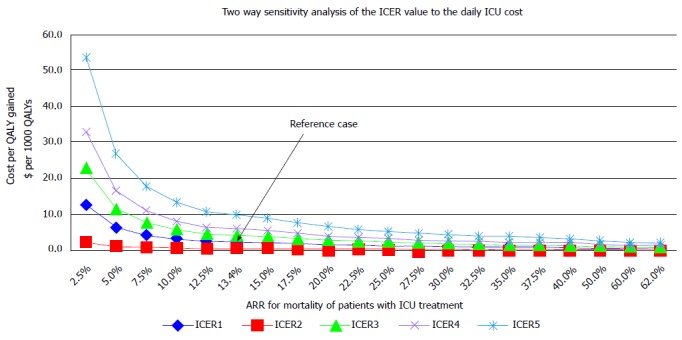
Methods: A prospective cohort study and economic evaluation of consecutive patients treated in a recently established medical ICU in Sarajevo, Bosnia and Herzegovina. A cost utility analysis of the intensive care of critically ill patients compared to the hospital ward treatment from the perspective of the health care system was subsequently performed. Incremental cost effectiveness was calculated using estimates of ICU vs non-ICU treatment effectiveness based on a formal systematic review of published studies. Decision analytic modeling was used to compare treatment alternatives. Sensitivity analyses of the key model parameters were performed.
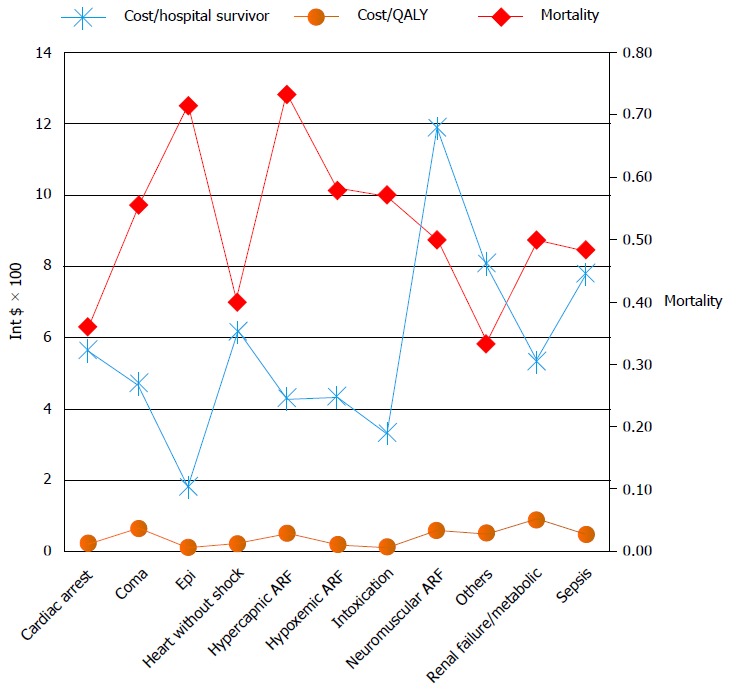
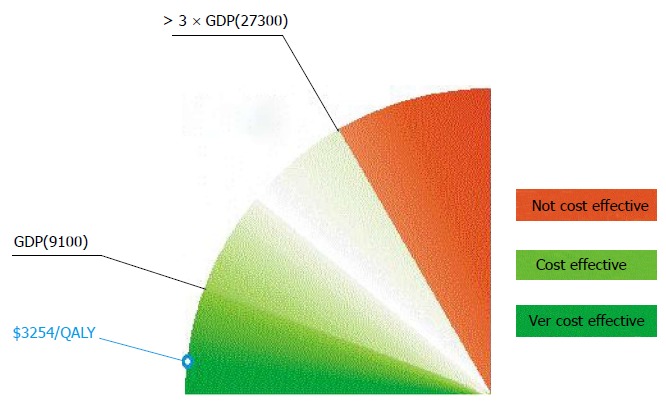
Results: Out of 148 patients, seventy patients (47.2%) survived to one year after critical illness with a median quality of life index 0.64 [interquartile range(IQR) 0.49-0.76]. Median number of life years gained per patient was 30 (IQR 16-40) or 18 quality adjusted life years (QALYs) (IQR 7-28). The cost of treatment of critically ill patients varied between 1820 dollar and 20109 dollar per hospital survivor and between 100 dollar and 2514 dollar per QALY saved. Mean factors that influenced costs were: Age, diagnostic category, ICU and hospital length of stay and number and type of diagnostic and therapeutic interventions. The incremental cost effectiveness ratio for ICU treatment was estimated at 3254 dollar per QALY corresponding to 35% of per capita GDP or a Very Cost Effective category according to World Health Organization criteria.
Conclusion: The ICU treatment of critically ill medical patients in a resource poor country is cost effective and compares favorably with other medical interventions. Public health authorities in low and middle income countries should encourage development of critical care services.
Keywords: Cost benefit analysis; Decision analysis; Economics; Intensive care; Intensive care unit; Mortality; Quality of life.
Figures
References
-
- Russel LB, Siegel JE, Daniels N, Gold MR, Luce BR, Mandelblatt JS. Cost-effectiveness analysis as a guide to resource allocation in health: roles and limitations. In: Gold MR, Siegel JE, Russel LB, Weinstein MC. Cost-Effectiveness in Health and Medicine. Oxford University Press; 1996. pp. 3–24.
-
- Weinstein MC, Stason WB. Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med. 1977;296:716–721. - PubMed
-
- Basic types of economic evaluation. In: Drummond MF, Sculpher MJ, Torrance GW, O¡¯Brien BJ, Stoddart GL. Methods for the Economic Evaluation of Health Care Programmes. Oxford University Press, 2005: 7-26
-
- Cost Effectiveness Analysis: Introduction. CDC Econ Eval Tutorials (E). [updated 2013 Nov 22] Available from: http//www.cdc.gov/owcd/eet/costeffect2/fixed/1.html.
-
- Sukcharoen N. Basic Principles of Health Economics for Obstetricians and Gynecologists. Thai J Obstet Gynaecol. 2003;15:3–7.
LinkOut - more resources
Full Text Sources
Other Literature Sources
