

Pictilisib for oestrogen receptor-positive, aromatase inhibitor-resistant, advanced or metastatic breast cancer (FERGI): a randomised, double-blind, placebo-controlled, phase 2 trial
- PMID: 27155741
- PMCID: PMC5524539
- DOI: 10.1016/S1470-2045(16)00106-6
Pictilisib for oestrogen receptor-positive, aromatase inhibitor-resistant, advanced or metastatic breast cancer (FERGI): a randomised, double-blind, placebo-controlled, phase 2 trial
Abstract
Background: Inhibition of phosphatidylinositol 3-kinase (PI3K) is a promising approach to overcome resistance to endocrine therapy in breast cancer. Pictilisib is an oral inhibitor of multiple PI3K isoforms. The aim of this study is to establish if addition of pictilisib to fulvestrant can improve progression-free survival in oestrogen receptor-positive, endocrine-resistant breast cancer.
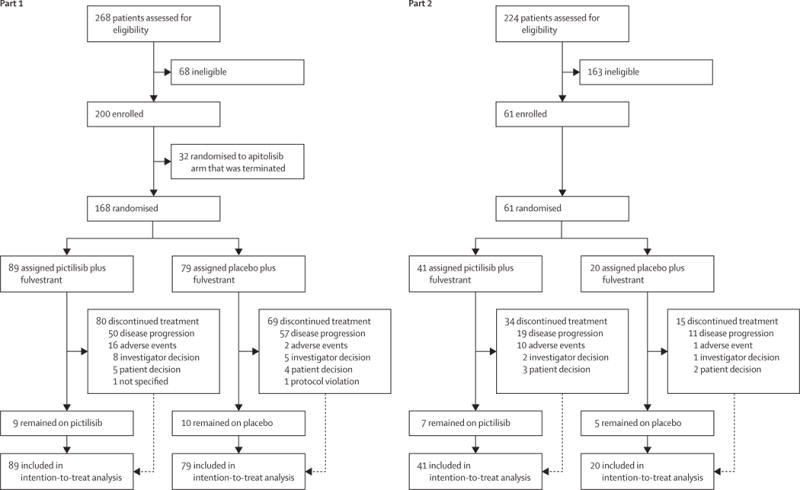
Methods: In this two-part, randomised, double-blind, placebo-controlled, phase 2 study, we recruited postmenopausal women aged 18 years or older with oestrogen receptor-positive, HER2-negative breast cancer resistant to treatment with an aromatase inhibitor in the adjuvant or metastatic setting, from 123 medical centres across 21 countries. Part 1 included patients with or without PIK3CA mutations, whereas part 2 included only patients with PIK3CA mutations. Patients were randomly allocated (1:1 in part 1 and 2:1 in part 2) via a computer-generated hierarchical randomisation algorithm to daily oral pictilisib (340 mg in part 1 and 260 mg in part 2) or placebo starting on day 15 of cycle 1, plus intramuscular fulvestrant 500 mg on day 1 and day 15 of cycle 1 and day 1 of subsequent cycles in both groups. In part 1, we stratified patients by presence or absence of PIK3CA mutation, primary or secondary aromatase inhibitor resistance, and measurable or non-measurable disease. In part 2, we stratified patients by previous aromatase inhibitor treatment for advanced or metastatic disease or relapse during or within 6 months of an aromatase inhibitor treatment in the adjuvant setting and measurable or non-measurable disease. All patients and those administering treatment and assessing outcomes were masked to treatment assignment. The primary endpoint was progression-free survival in the intention-to-treat population for both parts 1 and 2 and also separately in patients with PIK3CA-mutated tumours in part 1. Tumour assessment (physical examination and imaging scans) was investigator-assessed and done at screening and after 8 weeks, 16 weeks, 24 weeks, and 32 weeks of treatment from day 1 of cycle 1 and every 12 weeks thereafter. We assessed safety in as-treated patients who received at least one dose of study medication. This trial is registered with ClinicalTrials.gov, number NCT01437566.
Findings: In part 1, between Sept 27, 2011, and Jan 11, 2013, we randomly allocated 168 patients to the pictilisib (89 [53%]) or placebo (79 [47%]) group. In part 2, between March 18, 2013, and Jan 2, 2014, we randomly allocated 61 patients to the pictilisib (41 [67%]) or placebo (20 [33%]) group. In part 1, we found no difference in median progression-free survival between the pictilisib (6·6 months [95% CI 3·9-9·8]) and placebo (5·1 months [3·6-7·3]) group (hazard ratio [HR] 0·74 [95% CI 0·52-1·06]; p=0·096). We also found no difference when patients were analysed according to presence (pictilisib 6·5 months [95% CI 3·7-9·8] vs placebo 5·1 months [2·6-10·4]; HR 0·73 [95% CI 0·42-1·28]; p=0·268) or absence (5·8 months [3·6-11·1] vs 3·6 months [2·8-7·3]; HR 0·72 [0·42-1·23]; p=0·23) of PIK3CA mutation. In part 2, we also found no difference in progression-free survival between groups (5·4 months [95% CI 3·8-8·3] vs 10·0 months [3·6-13·0]; HR 1·07 [95% CI 0·53-2·18]; p=0·84). In part 1, grade 3 or worse adverse events occurred in 54 (61%) of 89 patients in the pictilisib group and 22 (28%) of 79 in the placebo group. 19 serious adverse events related to pictilisib treatment were reported in 14 (16%) of 89 patients. Only one (1%) of 79 patients reported treatment-related serious adverse events in the placebo group. In part 2, grade 3 or worse adverse events occurred in 15 (36%) of 42 patients in the pictilisib group and seven (37%) of 19 patients in the placebo group. Four serious adverse events related to pictilisib treatment were reported in two (5%) of 42 patients. One treatment-related serious adverse event occurred in one (5%) of 19 patients in the placebo group.
Interpretation: Although addition of pictilisib to fulvestrant did not significantly improve progression-free survival, dosing of pictilisib was limited by toxicity, potentially limiting its efficacy. For future assessment of PI3K inhibition as an approach to overcome resistance to hormonal therapy, inhibitors with greater selectivity than that of pictilisib might be needed to improve tolerability and potentially increase efficacy. No further investigation of pictilisib in this setting is ongoing.
Funding: F Hoffmann-La Roche.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
All other authors declare no competing interests.
Figures


Comment in
-
PI3K targeting in breast cancer: the end of the beginning?Lancet Oncol. 2016 Jun;17(6):696-697. doi: 10.1016/S1470-2045(16)00148-0. Epub 2016 May 4. Lancet Oncol. 2016. PMID: 27155742 No abstract available.
References
-
- Ring A, Dowsett M. Mechanisms of tamoxifen resistance. Endocr Relat Cancer. 2004;11:643–58. - PubMed
-
- Johnston SR. New strategies in estrogen receptor-positive breast cancer. Clin Cancer Res. 2010;16:1979–87. - PubMed
-
- Shou J, Massarweh S, Osborne CK, et al. Mechanisms of tamoxifen resistance: increased estrogen receptor-HER2/neu cross-talk in ER/HER2-positive breast cancer. J Natl Cancer Inst. 2004;96:926–35. - PubMed
-
- Baselga J, Semiglazov V, van Dam P, et al. Phase II randomized study of neoadjuvant everolimus plus letrozole compared with placebo plus letrozole in patients with estrogen receptor-positive breast cancer. J Clin Oncol. 2009;27:2630–37. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
