

Vegetarianism and cardiometabolic disease risk factors: Differences between South Asian and US adults
- PMID: 27155957
- PMCID: PMC4967403
- DOI: 10.1016/j.nut.2016.02.011
Vegetarianism and cardiometabolic disease risk factors: Differences between South Asian and US adults
Abstract
Objectives: Cardiometabolic diseases are increasing disproportionately in South Asia compared with other regions of the world despite high levels of vegetarianism. This unexpected discordance may be explained by differences in the healthfulness of vegetarian and non-vegetarian diets in South Asia compared with the United States. The aim of this study was to compare the food group intake of vegetarians with non-vegetarians in South Asia and the United States and to evaluate associations between vegetarianism and cardiometabolic disease risk factors (overweight/obesity, central obesity, diabetes, hypertension, high triacylglycerols, high low-density lipoprotein, low high-density lipoprotein, and high Framingham Heart Score).
Methods: Using cross-sectional data from adults (age 20-69 y) in South Asia (Centre for Cardiometabolic Risk Reduction in South-Asia [CARRS] 2010-2011; N = 15 665) and the United States (National Health and Nutrition Examination Survey 2003-2006; N = 2159), adherence to a vegetarian diet was assessed using food propensity questionnaires. Multivariable logistic regression was used to estimate odds ratios and predicted margins (e.g., adjusted prevalence of the outcomes).
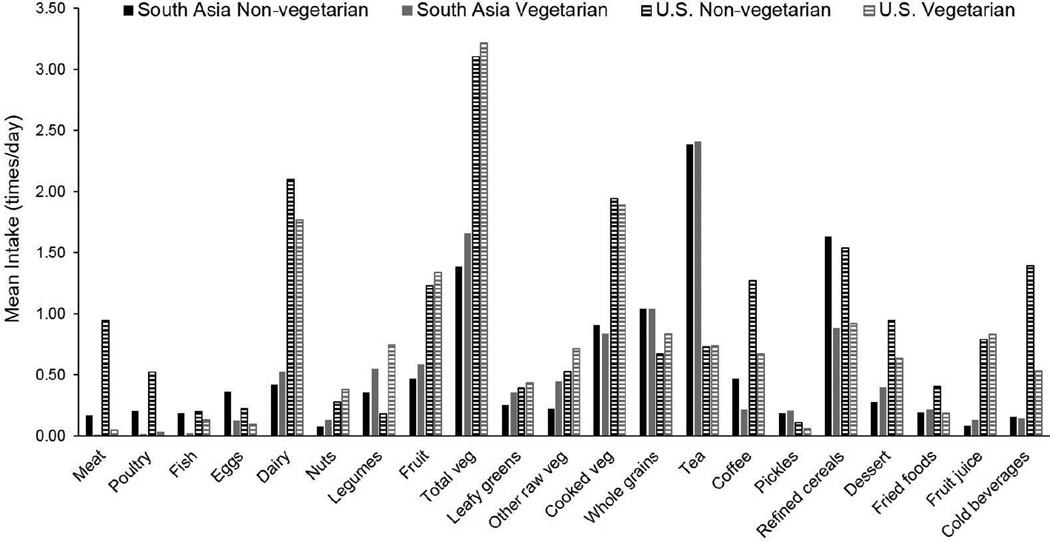
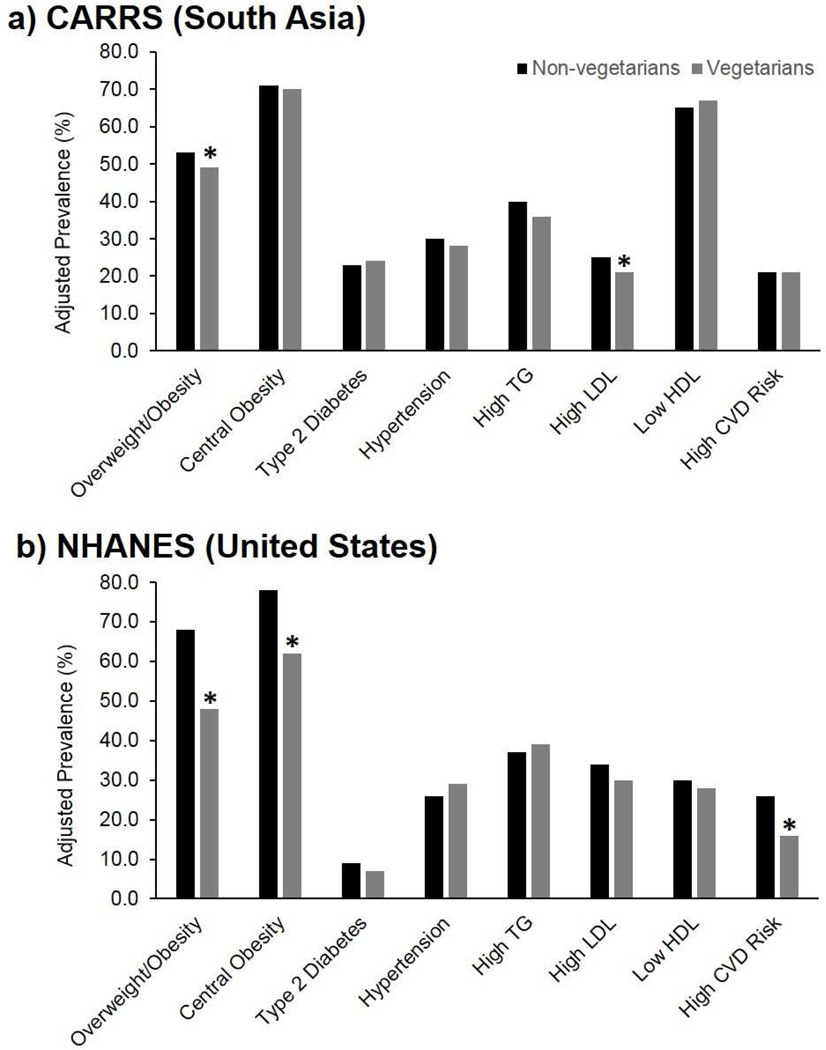
Results: One-third (33%; n = 4968) of adults in the South Asian sample were vegetarian compared with only 2.4% (n = 59) in the US sample. Among South Asians, vegetarians more frequently ate dairy, legumes, vegetables, fruit, desserts, and fried foods than non-vegitarians (all P < 0.05). Among Americans, vegetarians more frequently ate legumes, fruit, and whole grains, and less frequently ate refined cereals, desserts, fried foods, fruit juice, and soft drinks than non-vegetarians (all P < 0.05). After adjustment for confounders (age, sex, education, tobacco, alcohol, and also city in CARRS), South Asian vegetarians were slightly less frequently overweight/obese compared with non-vegetarians: 49% (95% confidence interval [CI], 45%-53%) versus 53% (95% CI, 51%-56%), respectively; whereas US vegetarians were considerably less frequently overweight/obese compared with non-vegetarians: 48% (95% CI, 32%-63%) versus 68% (95% CI, 65%-70%), respectively. Furthermore, US vegetarians were less likely to exhibit central obesity than non-vegetarians: 62% (95% CI, 43%-78%) versus 78% (95% CI, 76%-80%), respectively.
Conclusions: There is greater divergence between vegetarian and non-vegetarian diets in the United States than in South Asia, and US vegetarians have more consistently healthier food group intakes than South Asian vegetarians. Vegetarians in both populations have a lower probability of overweight/obesity compared with non-vegetarians. The strength of this association may be stronger for US vegetarian diets, which were also protective against central obesity.
Keywords: Food groups; India; Obesity; Vegetarianism; Visceral adiposity.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: None.
Figures
References
-
- Anjana R, Pradeepa R, Deepa M, et al. Prevalence of Diabetes and Prediabetes (Impaired Fasting Glucose and/or Impaired Glucose Tolerance) in Urban and Rural India: Phase I Results of the Indian Council of Medical Research–India Diabetes (ICMR–Indiab) Study. Diabetologia. 2011;54:3022–3027. - PubMed
-
- Guariguata L, Whiting DR, Hambleton I, et al. Global Estimates of Diabetes Prevalence for 2013 and Projections for 2035. Diabetes Res Clin Pract. 2014;103:137–149. - PubMed
-
- Gupta R. Burden of Coronary Heart Disease in India. Indian Heart J. 2004;57:632–638. - PubMed
-
- Gaziano T, Reddy KS, Paccaud F, et al. Cardiovascular Disease. Chapter 33. In: Jamison DT, Breman JG, Measham AR, et al., editors. Source: Disease Control Priorities in Developing Countries. 2nd. Washington (DC): World Bank; 2006. 2006. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
