

Gender differences in cannabis use disorder treatment: Change readiness and taking steps predict worse cannabis outcomes for women
- PMID: 27156221
- PMCID: PMC4884498
- DOI: 10.1016/j.addbeh.2016.04.014
Gender differences in cannabis use disorder treatment: Change readiness and taking steps predict worse cannabis outcomes for women
Abstract
Introduction: Gender differences in cannabis use and cannabis use disorder have been established. Regarding treatment, some evidence suggests that women are less responsive, though the mechanisms are not well understood. Motivation to change and self-efficacy are associated with better outcomes overall, and may help explain gender differences in cannabis use outcomes.
Methods: A secondary data analysis of a double-blind placebo controlled trial of buspirone treatment for cannabis dependence (N=175) was conducted. Self-report assessments of motivation to change, self-efficacy, and other clinical correlates were completed at baseline, and cannabis use was measured throughout the study.
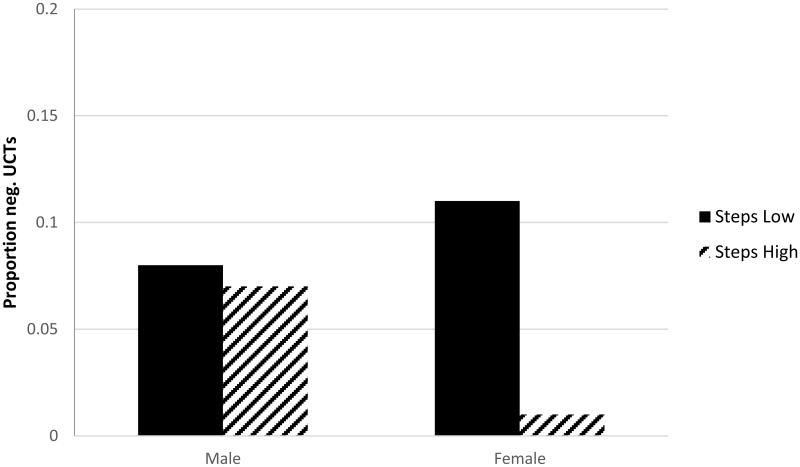
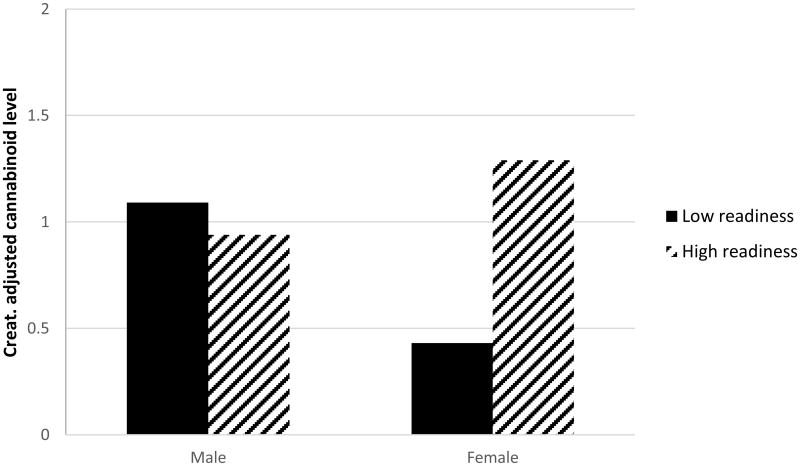
Results: There was a significant interaction between gender and taking steps on abstinence. Counter to hypothesis, higher taking steps reduced likelihood of achieving abstinence among women; there was no association among men. Subsequently, taking steps was associated with self-efficacy and quantity of use among men, and cannabis related problems among women. There was a significant interaction between gender and readiness to change on creatinine adjusted cannabinoid levels. Change readiness was positively associated with cannabinoid levels among women, but not men.
Conclusions: Motivation to change and initiation of change behavior predict worse cannabis outcomes in women. Men and women differ in what motivates change behavior. Social desirability, neurobiology, and treatment type may impact these effects. Gender differences in cannabis use and treatment responsiveness must be considered in future studies.
Keywords: Cannabis; Gender; Motivation; Sex differences; Taking steps; Treatment.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
