

Coexistence of lung cancer and immunoglobulin G4-related lung disease in a nodule: a case report
- PMID: 27156948
- PMCID: PMC4860762
- DOI: 10.1186/s13256-016-0898-3
Coexistence of lung cancer and immunoglobulin G4-related lung disease in a nodule: a case report
Abstract
Background: Immunoglobulin G4-related disease is characterized by infiltration of immunoglobulin G4-positive plasmacytes in various organs. The radiological findings of lung involvement of immunoglobulin G4-related disease include hilar and mediastinal lymphadenopathies, thickness of bronchovascular bundles, peribronchovascular consolidation, and lung nodules. Although a pathological approach is needed to diagnose immunoglobulin G4-related disease, it is ordinarily diagnosed by biopsy from one lesion even if there are multiple lesions. We reported a rare case of the coexistence of immunoglobulin G4-related disease and lung cancer in the same lung nodule.
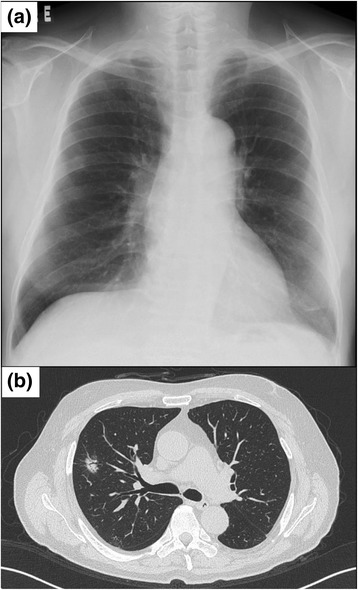
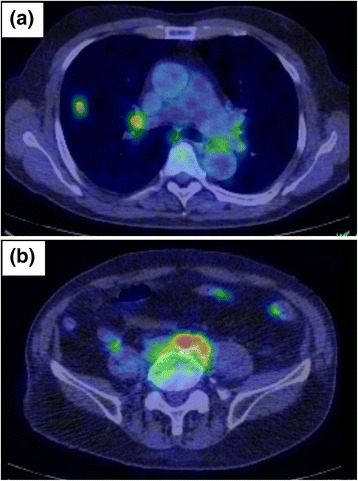
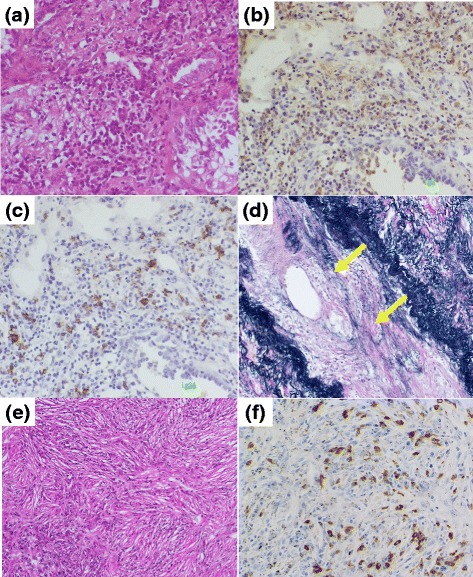
Case presentation: A 72-year-old Japanese man visited our hospital for evaluation of a nodular shadow in the middle lobe of his right lung that was seen on chest radiograph and computed tomography scan. An abdominal computed tomography scan showed a tumefactive lesion in his anterior sacral spine. Blood examinations revealed high serum immunoglobulin G4 concentration at 346 mg/dl, renal dysfunction, and anemia. He underwent right upper lobectomy and regional lymph node dissection. Pathologic findings of the lung nodule showed lepidic pattern adenocarcinoma with infiltration of immunoglobulin G4-positive plasma cells and obliterative phlebitis.
Conclusions: To date, there have been only few reports on the coexistence of immunoglobulin G4-related disease and lung cancer; here, we report such a rare case. Histologic examination should be considered in cases of suspicious immunoglobulin G4-related disease appearing in a lung nodule.
Keywords: IgG4-related disease; Lung cancer; Lung nodule.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
