

Risk factors and biomarkers of age-related macular degeneration
- PMID: 27156982
- PMCID: PMC4992630
- DOI: 10.1016/j.preteyeres.2016.04.003
Risk factors and biomarkers of age-related macular degeneration
Abstract
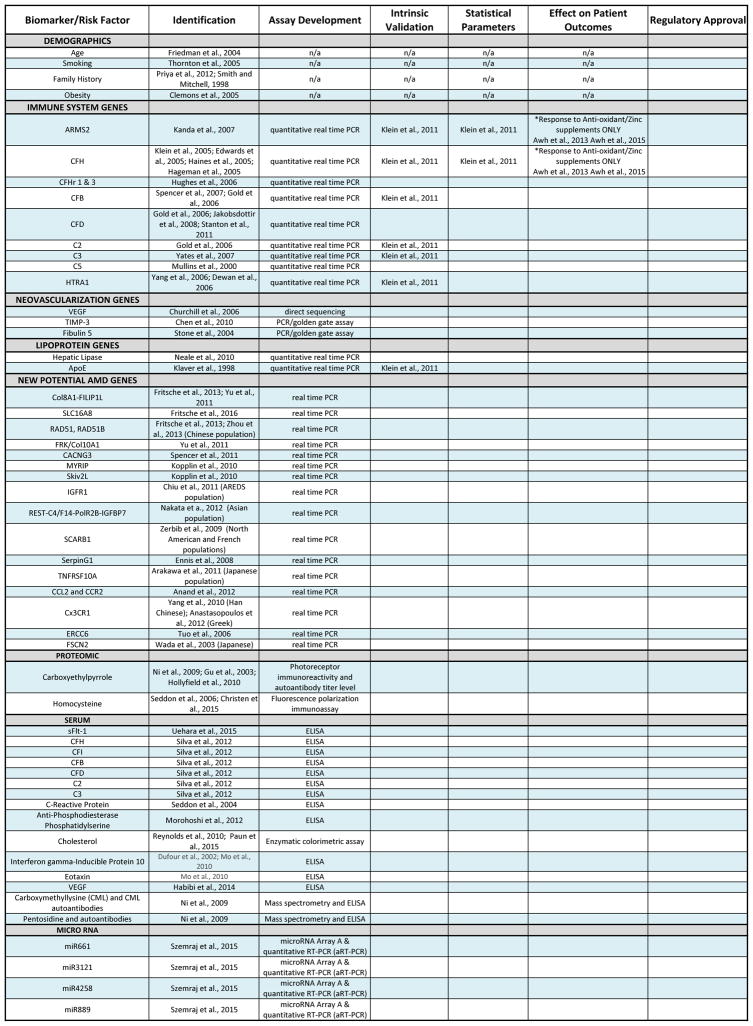
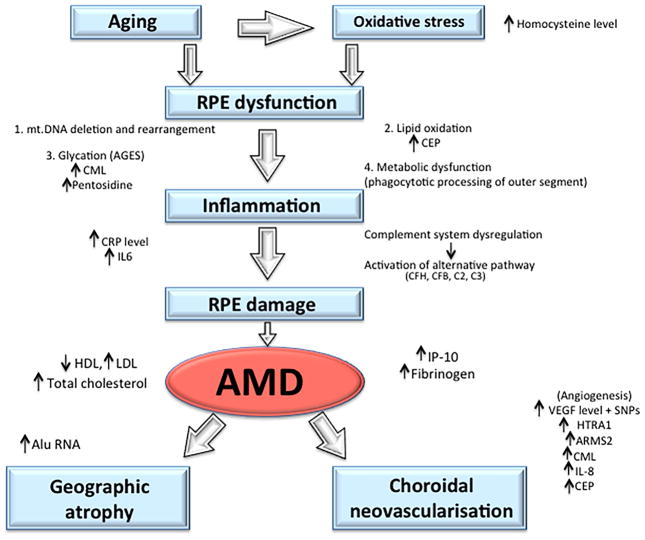
A biomarker can be a substance or structure measured in body parts, fluids or products that can affect or predict disease incidence. As age-related macular degeneration (AMD) is the leading cause of blindness in the developed world, much research and effort has been invested in the identification of different biomarkers to predict disease incidence, identify at risk individuals, elucidate causative pathophysiological etiologies, guide screening, monitoring and treatment parameters, and predict disease outcomes. To date, a host of genetic, environmental, proteomic, and cellular targets have been identified as both risk factors and potential biomarkers for AMD. Despite this, their use has been confined to research settings and has not yet crossed into the clinical arena. A greater understanding of these factors and their use as potential biomarkers for AMD can guide future research and clinical practice. This article will discuss known risk factors and novel, potential biomarkers of AMD in addition to their application in both academic and clinical settings.
Keywords: Age-related macular degeneration; Biomarkers; Proteomics; microRNA; sFlt.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors have no proprietary interests or conflicts
Figures
References
-
- Abedi F, Wickremasinghe S, Richardson AJ, Makalic E, Schmidt DF, Sandhu SS, Baird PN, Guymer RH. Variants in the VEGFA gene and treatment outcome after anti-VEGF treatment for neovascular age-related macular degeneration. Ophthalmology. 2013;120:115–121. - PubMed
-
- Abu-Safieh L, Abboud EB, Alkuraya H, Shamseldin H, Al-Enzi S, Al-Abdi L, Hashem M, Colak D, Jarallah A, Ahmad H, Bobis S, Nemer G, Bitar F, Alkuraya FS. Mutation of IGFBP7 causes upregulation of BRAF/MEK/ERK pathway and familial retinal arterial macroaneurysms. American journal of human genetics. 2011;89:313–319. - PMC - PubMed
-
- Adams MK, Simpson JA, Aung KZ, Makeyeva GA, Giles GG, English DR, Hopper J, Guymer RH, Baird PN, Robman LD. Abdominal obesity and age-related macular degeneration. American journal of epidemiology. 2011;173:1246–1255. - PubMed
-
- Adams MK, Simpson JA, Richardson AJ, English DR, Aung KZ, Makeyeva GA, Guymer RH, Giles GG, Hopper J, Robman LD, Baird PN. Apolipoprotein E gene associations in age-related macular degeneration: the Melbourne Collaborative Cohort Study. American journal of epidemiology. 2012;175:511–518. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
