

Cutaneous Hyperpigmentation in Megaloblastic Anemia: a Five Year Retrospective Review
- PMID: 27158434
- PMCID: PMC4848022
- DOI: 10.4084/MJHID.2016.021
Cutaneous Hyperpigmentation in Megaloblastic Anemia: a Five Year Retrospective Review
Abstract
Background: Cutaneous hyperpigmentation is an often overlooked clinical sign in megaloblastic anemia (MA) which has been sporadically reported in the literature.
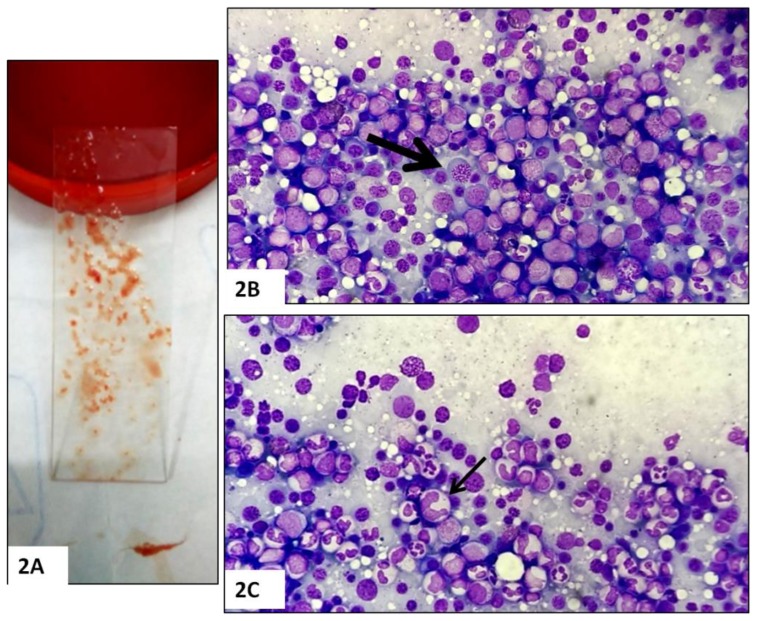
Methods: We describe the bone marrow (BM) changes and clinicolaboratory characteristics of 25 of 198 adult cases (>16 years) with cutaneous hyperpigmentation who underwent BM evaluation for cytopenia (s).
Results: Twenty-one of 25 cases (84%) had MA, while MA without hyperpigmentation occurred only in 12 of remainder 173 cases (P<0.001). Knuckle pad hyperpigmentation (KP) was noted in 16 (64%) cases; whereas 9 (36%) had diffuse brownish black discoloration (DP) of the palms and/or soles. Eighteen of 25 (72%) cases had pancytopenia (13 with KP) and 7 of 25 (28%) had bicytopenia (3 with KP). In addition, five cases (20%) presented with pyrexia. Of the 17 cases where data available, eleven were B12 deficient [<190 pg/ml; eight had severe deficiency (<100 pg/ml); ref.; 190-800pg/ml], while 4 had pure folate deficiency (< 4.0 ng/ml; ref.; 4-20ng/ml); and remainder 2 had combined B12 and folate deficiency. Compared to those with diffuse pigmentation; KP group had lower Hb (69.6 ± 24.2 vs. 86.3 ± 33.9 g/L), higher MCV (106.1 ±12.6 vs. 99.2 ± 7.6 fL), lower platelet count (50.9 ± 29.3 vs. 69.6 ± 36.5 × 10(9)/L), and lower median B12 [100.0 (30.0 - 822.0) vs. 316.0 (142.0 - 1617.3) pg/ml] (P>0.05). In six cases where follow-up data were available, there was a significant reversal of hyperpigmentation at 12 weeks following parenteral cobalamin therapy. In all five cases with pyrexia, fever subsided after 24 to 72 hours following administration of parenteral cobalamin therapy.
Conclusion: Cutaneous hyperpigmentation and cytopenia (s) are strongly associated with megaloblastic anemia. Knuckle pad hyperpigmentation is much more frequent than diffuse pigmentation of the palms and/or soles in such patents. A nonsignificant trend towards a greater degree of MA was found in cases with pigmentation of the knuckles.
Figures




References
-
- Hoffbrand AV. Megaloblastic anemias. In: Fauci AS, Brunwald E, Kasper DL, et al., editors. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill; 2008. pp. 643–651.
-
- Khanduri U, Sharma A. Megaloblastic anemia: prevalence and causative factors. Natl Med J India. 2007;20:172–175. - PubMed
-
- Arora S, Singh B, Gupta VK, Venkatesan M. Burden of vitamin B12 deficiency in urban population in Delhi, India: A hospital based study. Int J Pharma Biosci. 2011;2:B521–B528.
LinkOut - more resources
Full Text Sources
Other Literature Sources