

Protection against malaria at 1 year and immune correlates following PfSPZ vaccination
- PMID: 27158907
- PMCID: PMC11294733
- DOI: 10.1038/nm.4110
Protection against malaria at 1 year and immune correlates following PfSPZ vaccination
Erratum in
-
Corrigendum: Protection against malaria at 1 year and immune correlates following PfSPZ vaccination.Nat Med. 2016 Jun 7;22(6):692. doi: 10.1038/nm0616-692c. Nat Med. 2016. PMID: 27270781 No abstract available.
Abstract
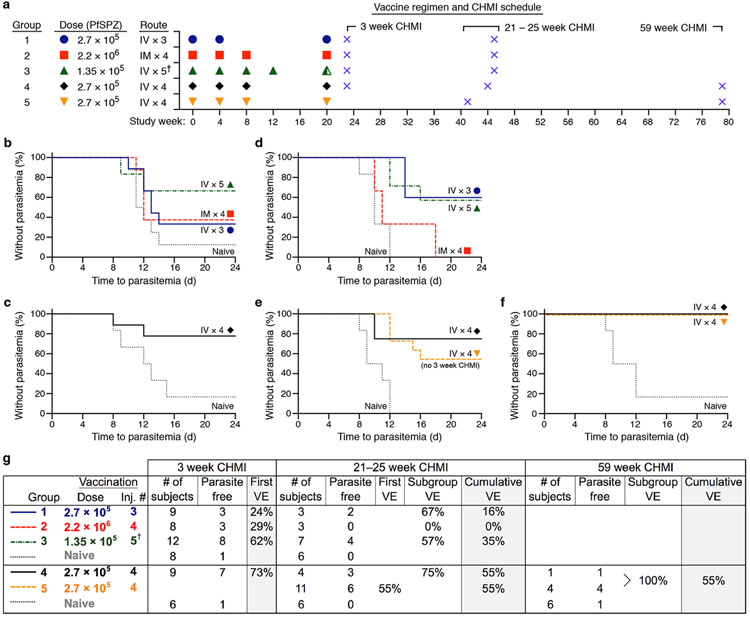
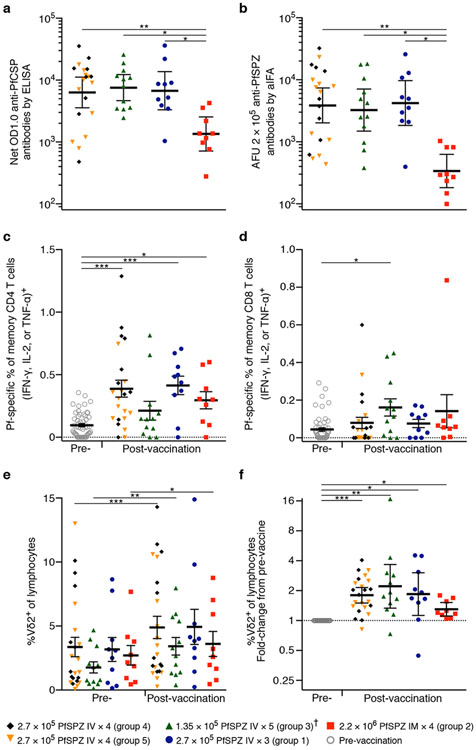
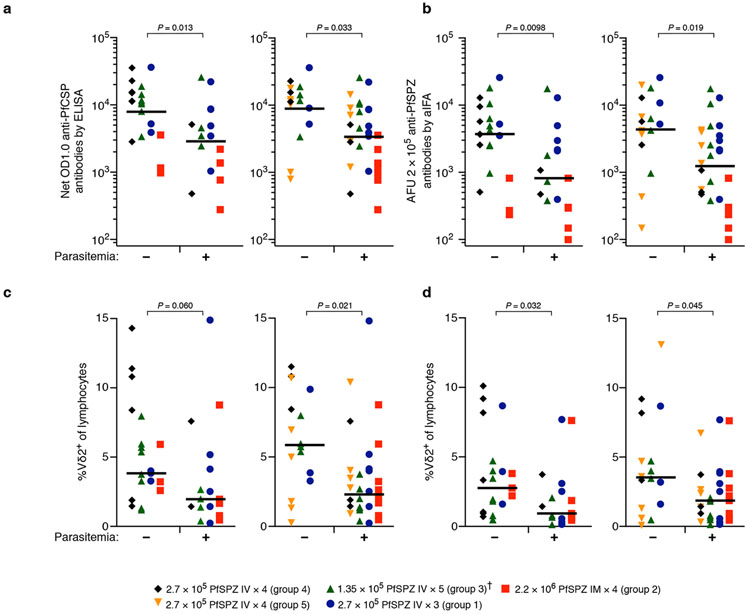
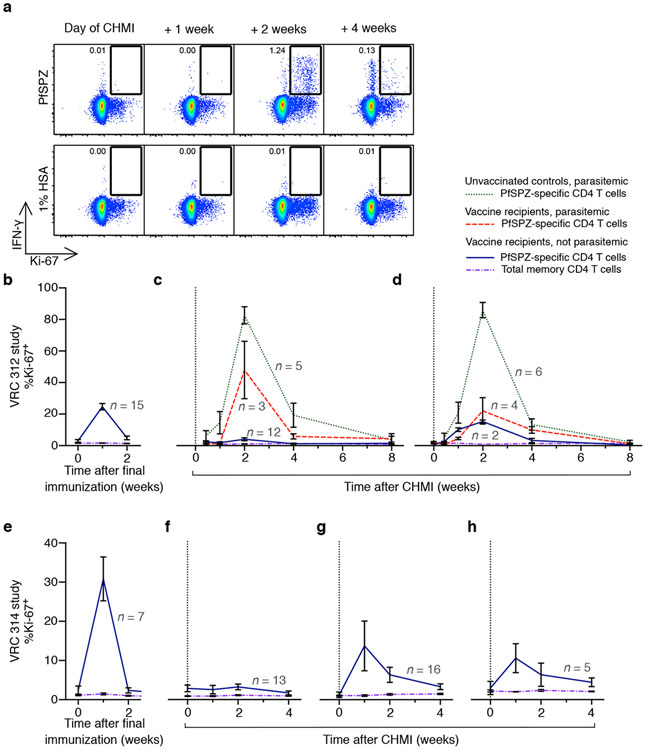
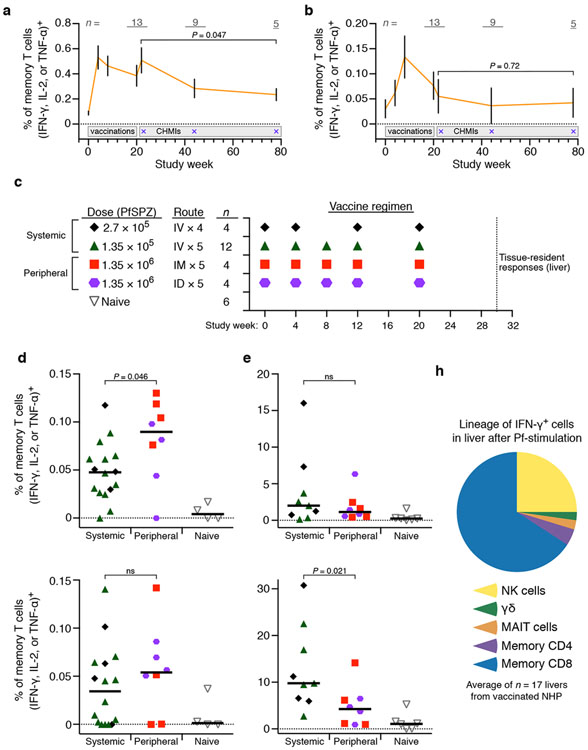
An attenuated Plasmodium falciparum (Pf) sporozoite (SPZ) vaccine, PfSPZ Vaccine, is highly protective against controlled human malaria infection (CHMI) 3 weeks after immunization, but the durability of protection is unknown. We assessed how vaccine dosage, regimen, and route of administration affected durable protection in malaria-naive adults. After four intravenous immunizations with 2.7 × 10(5) PfSPZ, 6/11 (55%) vaccinated subjects remained without parasitemia following CHMI 21 weeks after immunization. Five non-parasitemic subjects from this dosage group underwent repeat CHMI at 59 weeks, and none developed parasitemia. Although Pf-specific serum antibody levels correlated with protection up to 21-25 weeks after immunization, antibody levels waned substantially by 59 weeks. Pf-specific T cell responses also declined in blood by 59 weeks. To determine whether T cell responses in blood reflected responses in liver, we vaccinated nonhuman primates with PfSPZ Vaccine. Pf-specific interferon-γ-producing CD8 T cells were present at ∼100-fold higher frequencies in liver than in blood. Our findings suggest that PfSPZ Vaccine conferred durable protection to malaria through long-lived tissue-resident T cells and that administration of higher doses may further enhance protection.
Figures

References
REFERENCES FOR MAIN TEXT
-
- World Malaria Report 2015. (World Health Organization, 2015).
-
- Kester KE, et al. Randomized, double-blind, phase 2a trial of falciparum malaria vaccines RTS,S/AS01B and RTS,S/AS02A in malaria-naive adults: safety, efficacy, and immunologic associates of protection. The Journal of infectious diseases 200, 337–346 (2009). - PubMed
-
- Plowe CV, Alonso P & Hoffman SL The potential role of vaccines in the elimination of falciparum malaria and the eventual eradication of malaria. J Infect Dis 200, 1646–1649 (2009). - PubMed
METHODS-ONLY REFERENCES
-
- Chulay JD, et al. Malaria transmitted to humans by mosquitoes infected from cultured Plasmodium falciparum. Am J Trop Med Hyg 35, 66–68 (1986). - PubMed
-
- Rickman LS, et al. Plasmodium falciparum-infected Anopheles stephensi inconsistently transmit malaria to humans. Am J Trop Med Hyg 43, 441–445 (1990). - PubMed
-
- Lamoreaux L, Roederer M & Koup R Intracellular cytokine optimization and standard operating procedure. Nat Protoc 1, 1507–1516 (2006). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
