

Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study
- PMID: 27160187
- PMCID: PMC4861084
- DOI: 10.1136/bmj.i2214
Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study
Abstract
Objective: To determine the impact of the Hospital Value-Based Purchasing (HVBP) program-the US pay for performance program introduced by Medicare to incentivize higher quality care-on 30 day mortality for three incentivized conditions: acute myocardial infarction, heart failure, and pneumonia.
Design: Observational study.
Setting: 4267 acute care hospitals in the United States: 2919 participated in the HVBP program and 1348 were ineligible and used as controls (44 in general hospitals in Maryland and 1304 critical access hospitals across the United States).
Participants: 2 430 618 patients admitted to US hospitals from 2008 through 2013.
Main outcome measures: 30 day risk adjusted mortality for acute myocardial infarction, heart failure, and pneumonia using a patient level linear spline analysis to examine the association between the introduction of the HVBP program and 30 day mortality. Non-incentivized, medical conditions were the comparators. A secondary outcome measure was to determine whether the introduction of the HVBP program was particularly beneficial for a subgroup of hospital-poor performers at baseline-that may benefit the most.
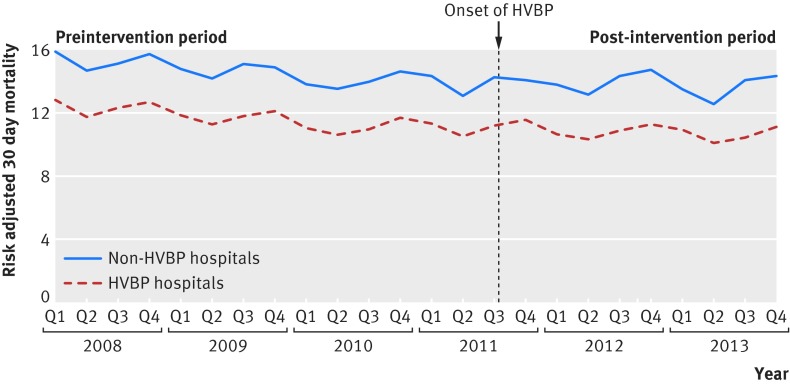
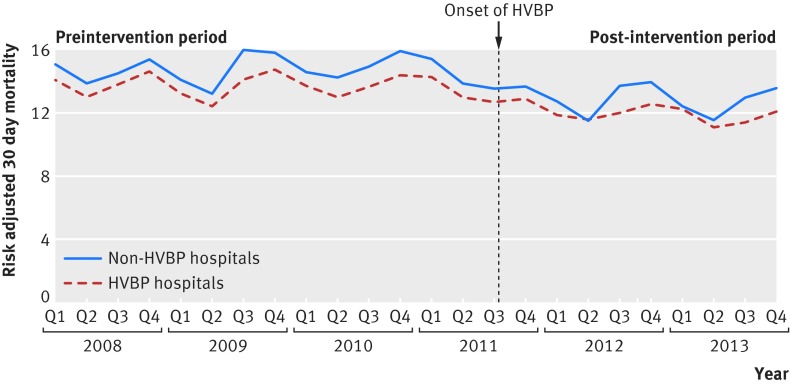
Results: Mortality rates of incentivized conditions in hospitals participating in the HVBP program declined at -0.13% for each quarter during the preintervention period and -0.03% point difference for each quarter during the post-intervention period. For non-HVBP hospitals, mortality rates declined at -0.14% point difference for each quarter during the preintervention period and -0.01% point difference for each quarter during the post-intervention period. The difference in the mortality trends between the two groups was small and non-significant (difference in difference in trends -0.03% point difference for each quarter, 95% confidence interval -0.08% to 0.13% point difference, P=0.35). In no subgroups of hospitals was HVBP associated with better outcomes, including poor performers at baseline.
Conclusions: Evidence that HVBP has led to lower mortality rates is lacking. Nations considering similar pay for performance programs may want to consider alternative models to achieve improved patient outcomes.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICJME uniform disclosure form at
Figures
Comment in
-
Should payment for performance depend on mortality?BMJ. 2016 Jun 22;353:i3429. doi: 10.1136/bmj.i3429. BMJ. 2016. PMID: 27335102 No abstract available.
References
-
- Kristensen SR, Bech M, Quentin W. A roadmap for comparing readmission policies with application to Denmark, England, Germany and the United States. Health Policy 2015;119:264-73. 10.1016/j.healthpol.2014.12.009 pmid:25547401. - DOI - PubMed
-
- Cashin C, Chi YL, Smith P, Borowitz M, Thomson S. Paying for Performance in Health Care: Implications for health system performance and accountability. 2014th Ed Open University Press. 2014.
-
- Cutler DM. Payment reform is about to become a reality. JAMA 2015;313:1606-7. 10.1001/jama.2015.1926 pmid:25919512. - DOI - PubMed
-
- Centers for Medicare Medicaid Services. Better Care. Smarter Spending. Healthier People: Paying Providers for Value, Not Volume. CMS.gov. 2015. Available from: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-....
-
- Burwell SM. Setting Value-Based Payment Goals—HHS Efforts to Improve U.S. Health Care. N Engl J Med 2015;372:897-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases