

Do spontaneous and mechanical breathing have similar effects on average transpulmonary and alveolar pressure? A clinical crossover study
- PMID: 27160458
- PMCID: PMC4862136
- DOI: 10.1186/s13054-016-1290-9
Do spontaneous and mechanical breathing have similar effects on average transpulmonary and alveolar pressure? A clinical crossover study
Abstract
Background: Preservation of spontaneous breathing (SB) is sometimes debated because it has potentially both negative and positive effects on lung injury in comparison with fully controlled mechanical ventilation (CMV). We wanted (1) to verify in mechanically ventilated patients if the change in transpulmonary pressure was similar between pressure support ventilation (PSV) and CMV for a similar tidal volume, (2) to estimate the influence of SB on alveolar pressure (Palv), and (3) to determine whether a reliable plateau pressure could be measured during pressure support ventilation (PSV).
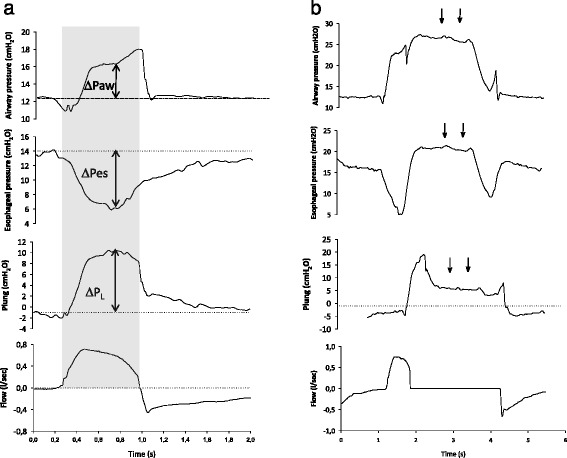
Methods: We studied ten patients equipped with esophageal catheters undergoing three levels of PSV followed by a phase of CMV. For each condition, we calculated the maximal and mean transpulmonary (ΔPL) swings and Palv.
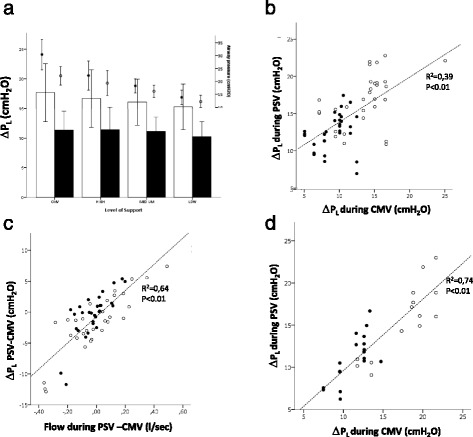
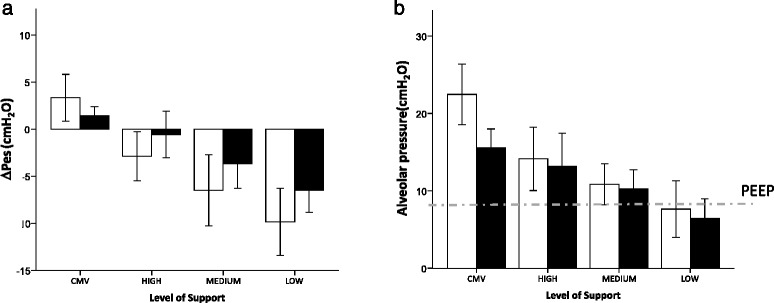
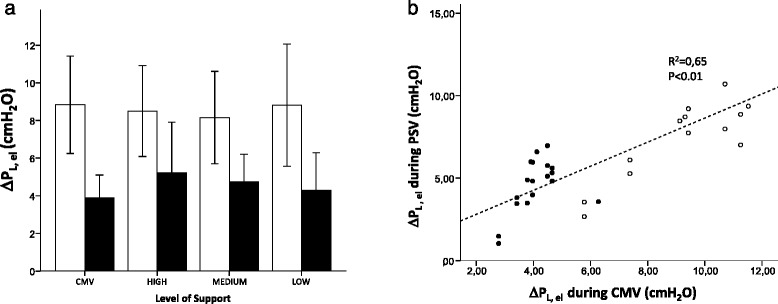
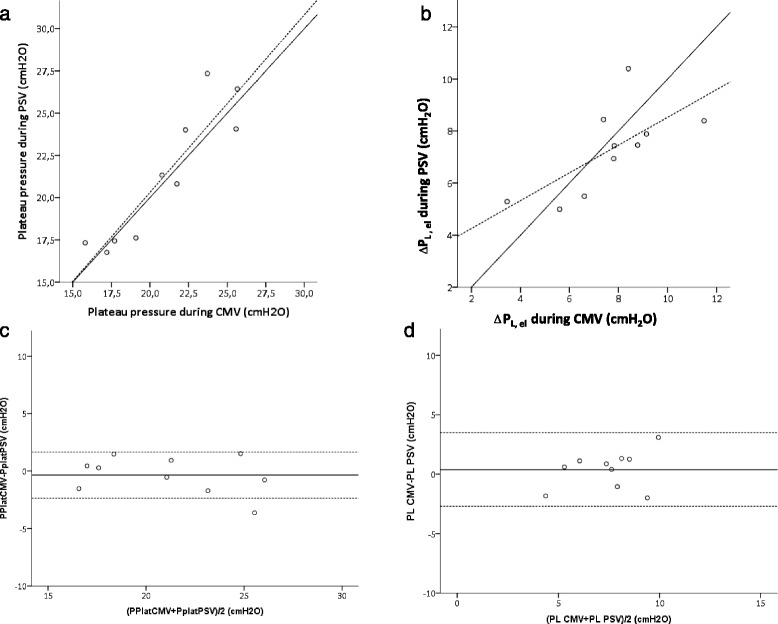
Results: Overall, ΔPL was similar between CMV and PSV, but only loosely correlated. The differences in ΔPL between CMV and PSV were explained largely by different inspiratory flows, indicating that the resistive pressure drop caused this difference. By contrast, the Palv profile was very different between CMV and SB; SB led to progressively more negative Palv during inspiration, and Palv became lower than the set positive end-expiratory pressure in nine of ten patients at low PSV. Finally, inspiratory occlusion holds performed during PSV led to plateau and Δ PL pressures comparable with those measured during CMV.
Conclusions: Under similar conditions of flow and volume, transpulmonary pressure change is similar between CMV and PSV. SB during mechanical ventilation can cause remarkably negative swings in Palv, a mechanism by which SB might potentially induce lung injury.
Keywords: Controlled ventilation; Esophageal pressure; Mechanical ventilation; Pressure support ventilation; Transpulmonary pressure.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
