

The distribution of ductal carcinoma in situ (DCIS) grade in 4232 women and its impact on overdiagnosis in breast cancer screening
- PMID: 27160733
- PMCID: PMC4862233
- DOI: 10.1186/s13058-016-0705-5
The distribution of ductal carcinoma in situ (DCIS) grade in 4232 women and its impact on overdiagnosis in breast cancer screening
Abstract
Background: The incidence of ductal carcinoma in situ (DCIS) has rapidly increased over time. The malignant potential of DCIS is dependent on its differentiation grade.
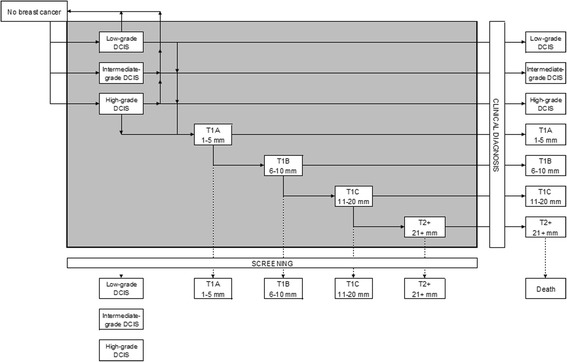
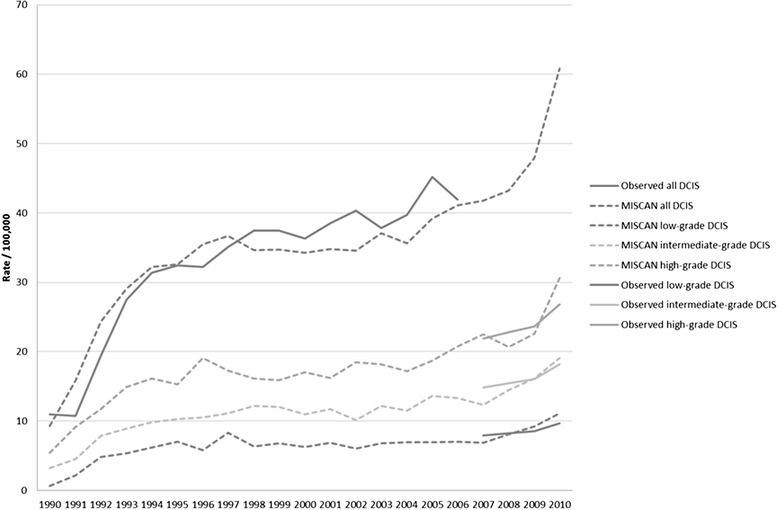
Methods: Our aim is to determine the distribution of different grades of DCIS among women screened in the mass screening programme, and women not screened in the mass screening programme, and to estimate the amount of overdiagnosis by grade of DCIS. We retrospectively included a population-based sample of 4232 women with a diagnosis of DCIS in the years 2007-2009 from the Nationwide network and registry of histopathology and cytopathology in the Netherlands. Excluded were women with concurrent invasive breast cancer, lobular carcinoma in situ and no DCIS, women recently treated for invasive breast cancer, no grade mentioned in the record, inconclusive record on invasion, and prevalent DCIS. The screening status was obtained via the screening organisations. The distribution of grades was incorporated in the well-established and validated microsimulation model MISCAN.
Results: Overall, 17.7 % of DCIS were low grade, 31.4 % intermediate grade, and 50.9 % high grade. This distribution did not differ by screening status, but did vary by age. Older women were more likely to have low-grade DCIS than younger women. Overdiagnosis as a proportion of all cancers in women of the screening age was 61 % for low-grade, 57 % for intermediate-grade, 45 % for high-grade DCIS. For women age 50-60 years with a high-grade DCIS this overdiagnosis rate was 21-29 %, compared to 50-66 % in women age 60-75 years with high-grade DCIS.
Conclusions: Amongst the rapidly increasing numbers of DCIS diagnosed each year is a significant number of overdiagnosed cases. Tailoring treatment to the probability of progression is the next step to preventing overtreatment. The basis of this tailoring could be DCIS grade and age.
Keywords: Breast cancer; Ductal carcinoma in situ; MISCAN; Overdiagnosis; Screening.
Figures

References
-
- Registry TNC. Cijfersoverkanker. 2013. http://www.cijfersoverkanker.nl. Accessed 17 Sept 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
