

Delayed cerebral ischaemia prevention and treatment after aneurysmal subarachnoid haemorrhage: a systematic review
- PMID: 27160932
- PMCID: PMC4913393
- DOI: 10.1093/bja/aew095
Delayed cerebral ischaemia prevention and treatment after aneurysmal subarachnoid haemorrhage: a systematic review
Abstract
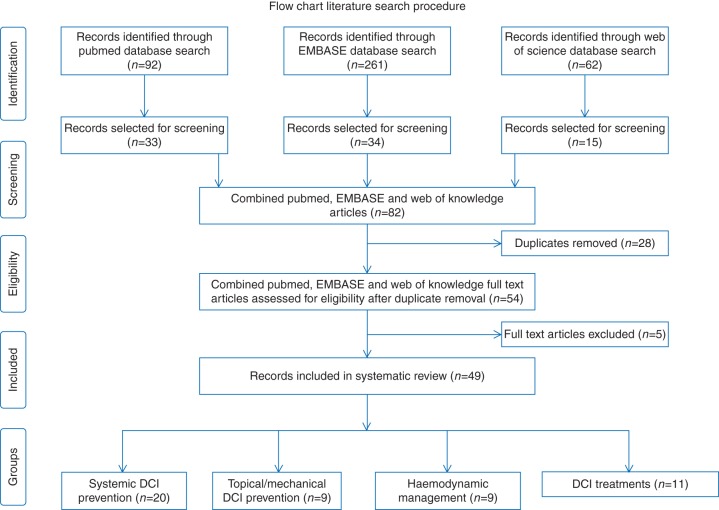
: The leading cause of morbidity and mortality after surviving the rupture of an intracranial aneurysm is delayed cerebral ischaemia (DCI). We present an update of recent literature on the current status of prevention and treatment strategies for DCI after aneurysmal subarachnoid haemorrhage. A systematic literature search of three databases (PubMed, ISI Web of Science, and Embase) was performed. Human clinical trials assessing treatment strategies, published in the last 5 yr, were included based on full-text analysis. Study data were extracted using tables depicting study type, sample size, and outcome variables. We identified 49 studies meeting our inclusion criteria. Clazosentan, magnesium, and simvastatin have been tested in large high-quality trials but failed to show a beneficial effect. Cilostazol, eicosapentaenoic acid, erythropoietin, heparin, and methylprednisolone yield promising results in smaller, non-randomized or retrospective studies and warrant further investigation. Topical application of nicardipine via implants after clipping has been shown to reduce clinical and angiographic vasospasm. Methods to improve subarachnoid blood clearance have been established, but their effect on outcome remains unclear. Haemodynamic management of DCI is evolving towards euvolaemic hypertension. Endovascular rescue therapies, such as percutaneous transluminal balloon angioplasty and intra-arterial spasmolysis, are able to resolve angiographic vasospasm, but their effect on outcome needs to be proved. Many novel therapies for preventing and treating DCI after aneurysmal subarachnoid haemorrhage have been assessed, with variable results. Limitations of the study designs often preclude definite statements. Current evidence does not support prophylactic use of clazosentan, magnesium, or simvastatin. Many strategies remain to be tested in larger randomized controlled trials.
Clinical trial registration: This systematic review was registered in the international prospective register of systematic reviews.
Prospero: CRD42015019817.
Keywords: brain ischaemia; subarachnoid haemorrhage; vasospasm, intracranial.
© The Author 2016. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007; 369: 306–18 - PubMed
-
- Rinkel GJ, Algra A. Long-term outcomes of patients with aneurysmal subarachnoid haemorrhage. Lancet Neurol 2011; 10: 349–56 - PubMed
-
- Dodel R, Winter Y, Ringel F et al. Cost of illness in subarachnoid hemorrhage: a German longitudinal study. Stroke 2010; 41: 2918–23 - PubMed
-
- Kassell NF, Torner JC, Jane JA, Haley EC Jr, Adams HP. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 2: surgical results. J Neurosurg 1990; 73: 37–47 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
