

Sex Differences in Cardiorespiratory Fitness and All-Cause Mortality: The Henry Ford ExercIse Testing (FIT) Project
- PMID: 27161032
- PMCID: PMC5617114
- DOI: 10.1016/j.mayocp.2016.04.002
Sex Differences in Cardiorespiratory Fitness and All-Cause Mortality: The Henry Ford ExercIse Testing (FIT) Project
Abstract
Objective: To determine whether sex modifies the relationship between fitness and mortality.
Patients and methods: We included 57,284 patients without coronary artery disease or heart failure who completed a routine treadmill exercise test between 1991 and 2009. We determined metabolic equivalent tasks (METs) and linked patient records with mortality data via the Social Security Death Index. Multivariable Cox regression was used to determine the association between sex, fitness, and all-cause mortality.
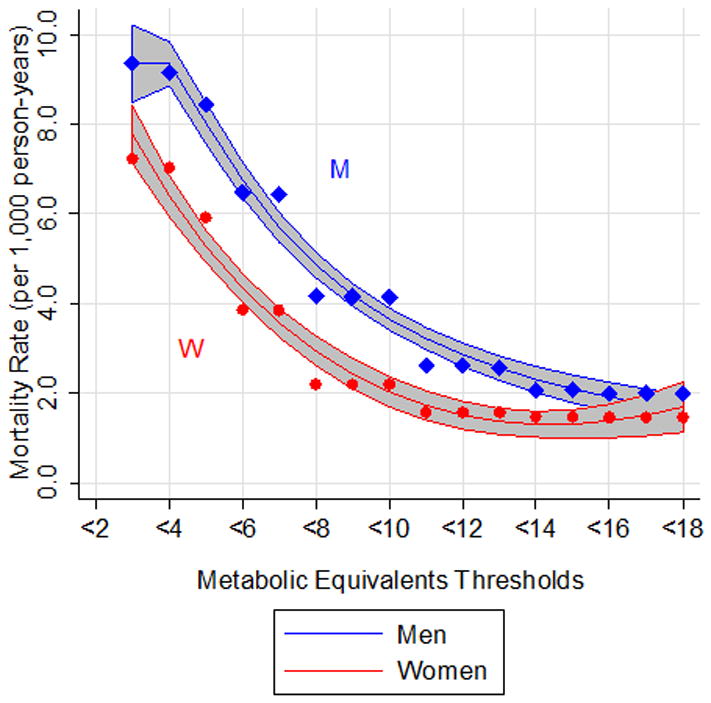
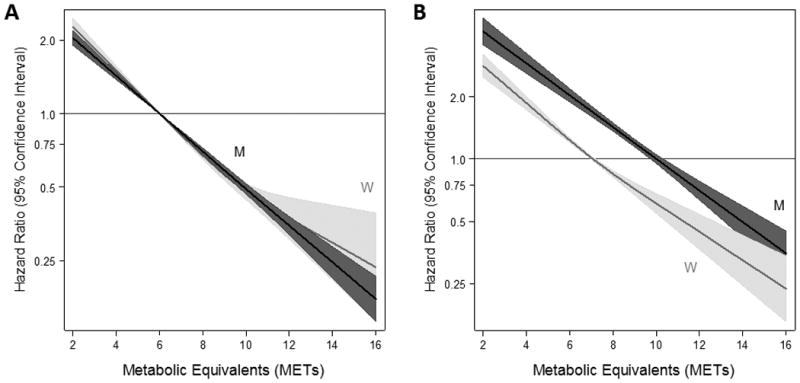
Results: There were 29,470 men (51.4%) and 27,814 women (48.6%) with mean ages of 53 and 54 years, respectively. Overall, men achieved 1.7 METs higher than women (P<.001). During median follow-up of 10 years, there were 6402 deaths. The mortality rate for men in each MET group was similar to that for women, who achieved an average of 2.6 METs lower (P=.004). Fitness was inversely associated with mortality in both men (hazard ratio [HR], 0.84 per 1 MET; 95% CI, 0.83-0.85) and women (HR, 0.83 per 1 MET; 95% CI, 0.81-0.84). This relationship did not plateau at high or low MET values.
Conclusion: Although men demonstrated 1.7 METs higher than women, their survival was equivalent to that of women demonstrating 2.6 METs lower. Furthermore, higher MET values were associated with lower mortality for both men and women across the range of MET values. These findings are useful for tailoring prognostic information and lifestyle guidance to men and women undergoing stress testing.
Copyright © 2016 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Bouchard C, An P, Rice T, et al. Familial aggregation of VO(2max) response to exercise training: results from the HERITAGE Family Study. J Appl Physiol. 1999;87(3):1003–1008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
