

Evaluating Cancer of the Central Nervous System Through Next-Generation Sequencing of Cerebrospinal Fluid
- PMID: 27161972
- PMCID: PMC4981784
- DOI: 10.1200/JCO.2016.66.6487
Evaluating Cancer of the Central Nervous System Through Next-Generation Sequencing of Cerebrospinal Fluid
Erratum in
-
Erratum.J Clin Oncol. 2017 Jun 10;35(17):1972. doi: 10.1200/JCO.2017.73.8708. J Clin Oncol. 2017. PMID: 28591544 Free PMC article. No abstract available.
Abstract
Purpose: Cancer spread to the central nervous system (CNS) often is diagnosed late and is unresponsive to therapy. Mechanisms of tumor dissemination and evolution within the CNS are largely unknown because of limited access to tumor tissue.
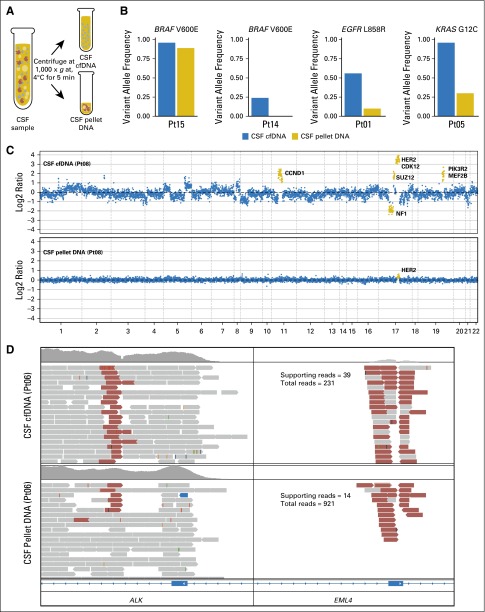
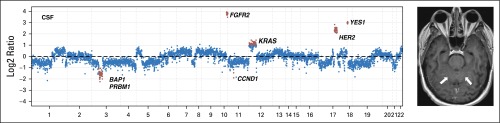
Materials and methods: We sequenced 341 cancer-associated genes in cell-free DNA from cerebrospinal fluid (CSF) obtained through routine lumbar puncture in 53 patients with suspected or known CNS involvement by cancer.
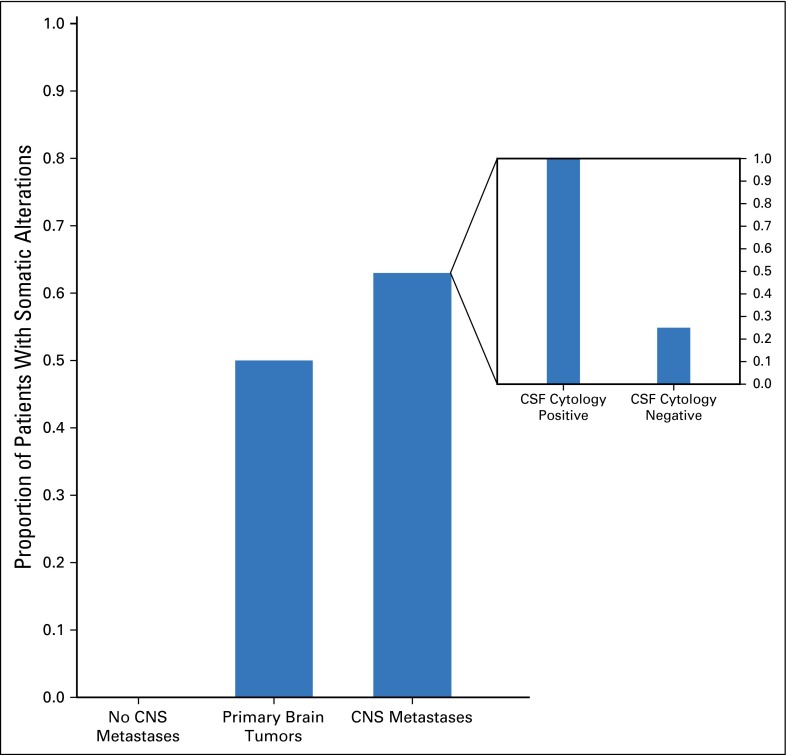
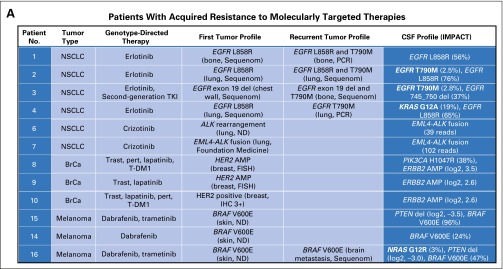
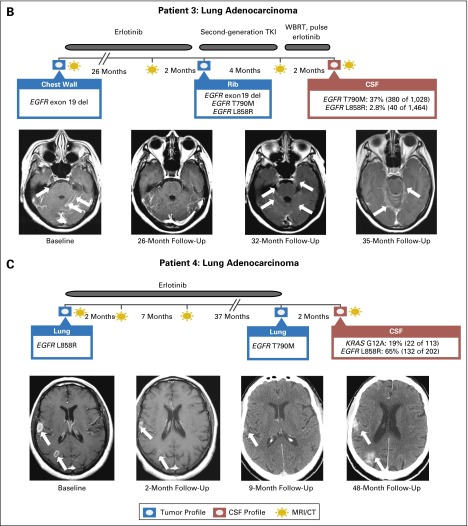
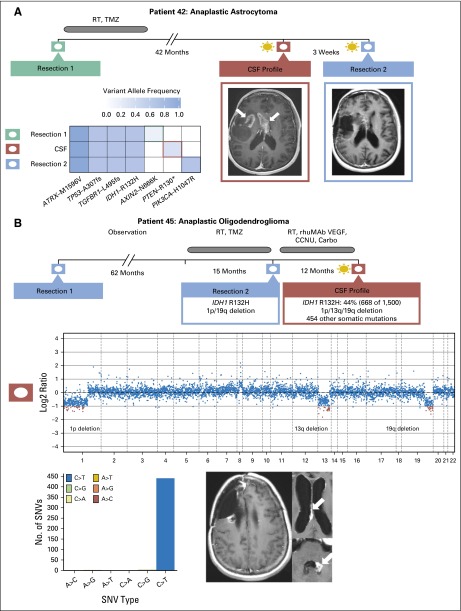
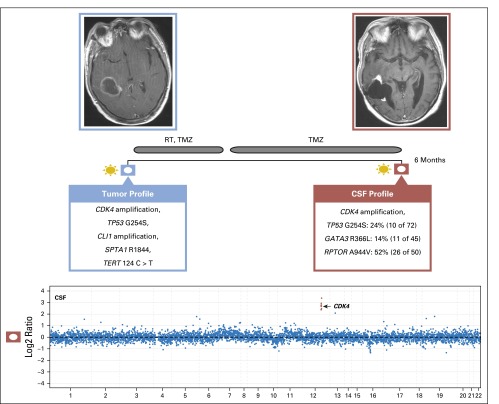
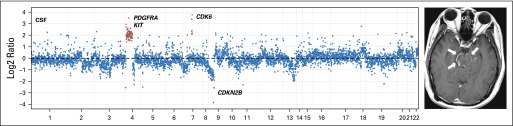
Results: We detected high-confidence somatic alterations in 63% (20 of 32) of patients with CNS metastases of solid tumors, 50% (six of 12) of patients with primary brain tumors, and 0% (zero of nine) of patients without CNS involvement by cancer. Several patients with tumor progression in the CNS during therapy with inhibitors of oncogenic kinases harbored mutations in the kinase target or kinase bypass pathways. In patients with glioma, the most common malignant primary brain tumor in adults, examination of cell-free DNA uncovered patterns of tumor evolution, including temozolomide-associated mutations.
Conclusion: The study shows that CSF harbors clinically relevant genomic alterations in patients with CNS cancers and should be considered for liquid biopsies to monitor tumor evolution in the CNS.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Haber DA, Gray NS, Baselga J. The evolving war on cancer. Cell. 2011;145:19–24. - PubMed
-
- Rhodes CH, Honsinger C, Sorenson GD. PCR-detection of tumor-derived p53 DNA in cerebrospinal fluid. Am J Clin Pathol. 1995;103:404–408. - PubMed
-
- Swinkels DW, de Kok JB, Hanselaar A, et al. Early detection of leptomeningeal metastasis by PCR examination of tumor-derived K-ras DNA in cerebrospinal fluid. Clin Chem. 2000;46:132–133. - PubMed
-
- Shingyoji M, Kageyama H, Sakaida T, et al. Detection of epithelial growth factor receptor mutations in cerebrospinal fluid from patients with lung adenocarcinoma suspected of neoplastic meningitis. J Thorac Oncol. 2011;6:1215–1220. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
