

The Diagnostic Dilemma of Primary Epiploic Appendagitis and How to Establish a Diagnosis
- PMID: 27162597
- PMCID: PMC4852085
- DOI: 10.5001/omj.2016.45
The Diagnostic Dilemma of Primary Epiploic Appendagitis and How to Establish a Diagnosis
Abstract
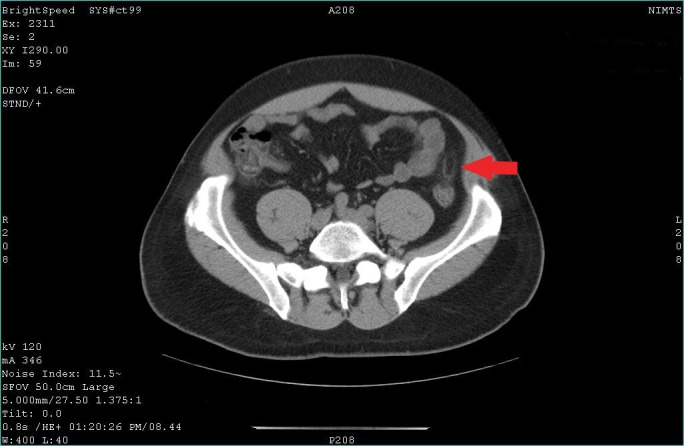
Primary epiploic appendagitis (PEA) is a relatively uncommon, non-surgical situation that clinically mimics other conditions requiring surgery. In PEA, torsion and inflammation of an epiploic appendix results in localized abdominal pain. This condition may be clinically misdiagnosed, resulting in unnecessary surgical intervention. We report the unusual case of a healthy 44-year-old man, who presented to the 417 NIMTS Military Veterans' Fund Hospital of Athens with non-migratory left lower quadrant abdominal pain, which had started 24 hours before admission. The patient described a constant, sharp, non-radiating pain. He had no symptoms of nausea, vomiting, constipation, diarrhea, or fever. Abdominal examination showed focal abdominal tenderness with slight rebound tenderness. The diagnosis of PEA of the sigmoid colon was made based on the findings of an abdominal contrast computed tomography (CT). The key findings of CT were an oval lesion with a maximum diameter of 2.4 cm, with fat attenuation, and a circumferential hyperdense ring located adjacent to the sigmoid colon. This case is presented to highlight the clinical characteristics of PEA, which may help clinicians to overcome this diagnostic dilemma and reach the correct diagnosis.
Keywords: Appendix Epiploica; Diagnosis; Inflammation; Radiology.
Figures
Similar articles
-
Right lower quadrant pain: not always appendicitis but epiploic appendagitis of appendix.Radiol Case Rep. 2021 Oct 2;16(12):3695-3697. doi: 10.1016/j.radcr.2021.08.069. eCollection 2021 Dec. Radiol Case Rep. 2021. PMID: 34630803 Free PMC article.
-
Primary Epiploic Appendagitis of the Appendix Vermiformis.Curr Med Imaging. 2023;19(10):1207-1209. doi: 10.2174/1573405618666220816103122. Curr Med Imaging. 2023. PMID: 35975863
-
Primary Epiploic Appendagitis: A Mimicker of Abdominal Pain.Clin Med Res. 2023 Sep;21(3):159-162. doi: 10.3121/cmr.2023.1837. Clin Med Res. 2023. PMID: 37985168 Free PMC article.
-
Acute epiploic appendagitis and its mimics.Radiographics. 2005 Nov-Dec;25(6):1521-34. doi: 10.1148/rg.256055030. Radiographics. 2005. PMID: 16284132 Review.
-
Epiploic appendagitis: pathogenesis, clinical findings and imaging clues of a misdiagnosed mimicker.Ann Transl Med. 2019 Dec;7(24):814. doi: 10.21037/atm.2019.12.74. Ann Transl Med. 2019. PMID: 32042830 Free PMC article. Review.
Cited by
-
Acute Epiploic Appendagitis: A Nonsurgical Abdominal Pain.Case Rep Emerg Med. 2019 Jul 14;2019:7160247. doi: 10.1155/2019/7160247. eCollection 2019. Case Rep Emerg Med. 2019. PMID: 31380126 Free PMC article.
-
Bilateral Epiploic Appendagitis: A Rather Benign but Diagnostically Challenging Cause of Acute Abdominal Pain.Cureus. 2020 Apr 30;12(4):e7897. doi: 10.7759/cureus.7897. Cureus. 2020. PMID: 32494512 Free PMC article.
-
Acute epiploic appendigitis: Diagnostic and laparoscopic approach.Int J Surg Case Rep. 2018;44:157-160. doi: 10.1016/j.ijscr.2018.02.003. Epub 2018 Feb 23. Int J Surg Case Rep. 2018. PMID: 29505992 Free PMC article.
-
Variable Radiological Presentations of Acute Appendicitis With Epiploic Appendagitis as a Differential Diagnosis: A Case Series.Cureus. 2025 Jun 4;17(6):e85381. doi: 10.7759/cureus.85381. eCollection 2025 Jun. Cureus. 2025. PMID: 40621289 Free PMC article.
-
Primary epiploic appendagitis as an unusual cause of acute abdominal pain in a middle-aged male: A case report.Medicine (Baltimore). 2019 Aug;98(33):e16846. doi: 10.1097/MD.0000000000016846. Medicine (Baltimore). 2019. PMID: 31415410 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources