

Effect of parecoxib combined with thoracic epidural analgesia on pain after thoracotomy
- PMID: 27162662
- PMCID: PMC4842798
- DOI: 10.21037/jtd.2016.03.45
Effect of parecoxib combined with thoracic epidural analgesia on pain after thoracotomy
Abstract
Background: Thoracotomy results in severe postoperative pain potentially leading to chronic pain. We investigated the potential benefits of intravenous parecoxib on postoperative analgesia combined with thoracic epidural analgesia (TEA).
Methods: Eighty-six patients undergoing thoracic surgery were randomized into two groups. Patient-controlled epidural analgesia (PCEA) was used until chest tubes were removed. Patients received parecoxib (group P) or placebo (group C) intravenously just 0.5 h before the operation and every 12 h after operation for 3 days. The intensity of pain was measured by using a visual analogue scale (VAS) and recorded at 2, 4, 8, 24, 48, 72 h after operation. The valid number of PCA, the side effects and the overall satisfaction to analgesic therapy in 72 h were recorded. Venous blood samples were taken before operation, the 1(st) and 3(rd) day after operation for plasma cortisol, adrenocorticotropic hormone (ACTH), interleukin-6 and tumor necrosis factor-α level. The occurrence of residual pain was recorded using telephone questionnaire 2 and 12 months after surgery.
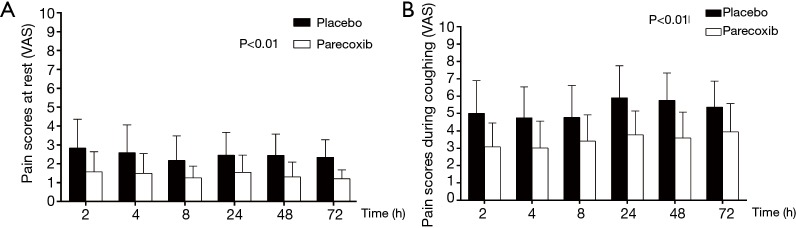
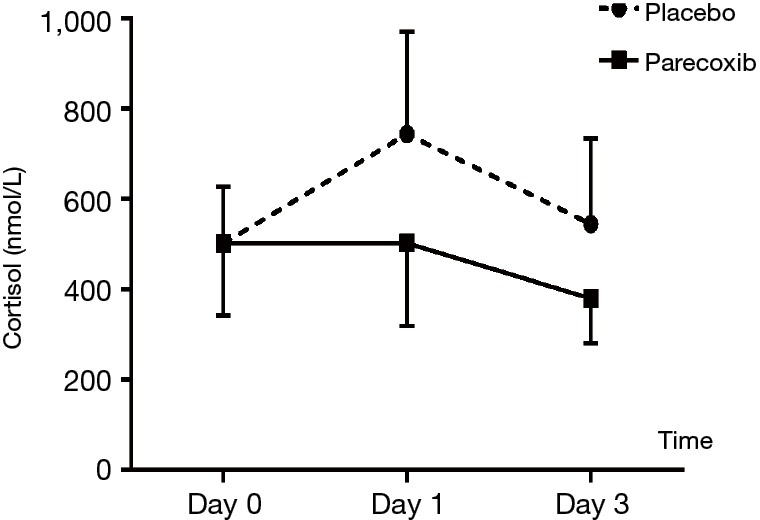
Results: Postoperative pain scores at rest and on coughing were significantly lower with the less valid count of PCA and greater patient satisfaction in group P (P<0.01). Adverse effect and the days fit for discharge were comparable between two groups. The cortisol levels in placebo group were higher than parecoxib group at T2. The level of ACTH both decreased in two groups after operation but it was significantly lower in group P than that in group C. There were no changes in plasma IL-6 and TNF-α levels before and after analgesia at T1 and T2 (P>0.05). The occurrence of residual pain were 25% and 51.2% separately in group P and C 3 months postoperatively (P<0.05).
Conclusions: Intravenous parecoxib in multimodal analgesia improves postoperative analgesia provided by TEA, relieves stress response after thoracotomy, and may restrain the development of chronic pain.
Keywords: Epidural analgesia; parecoxib; postoperative analgesia; thoracotomy.
Conflict of interest statement
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous