

Teardrop fracture following head-first impact in an ice hockey player: Case report and analysis of injury mechanisms
- PMID: 27162711
- PMCID: PMC4852594
- DOI: 10.14444/3009
Teardrop fracture following head-first impact in an ice hockey player: Case report and analysis of injury mechanisms
Abstract
Background: We report a case of a young male athlete who sustained a three column displaced teardrop fracture of the C5 vertebra due to a head-first impact in hockey, suffered neurapraxia, yet made full neurological recovery. This full recovery was in sharp contrast to multiple case series which reported permanent quadriplegia in the vast majority of teardrop fracture patients. We investigate the etiology and biomechanical mechanisms of injury.
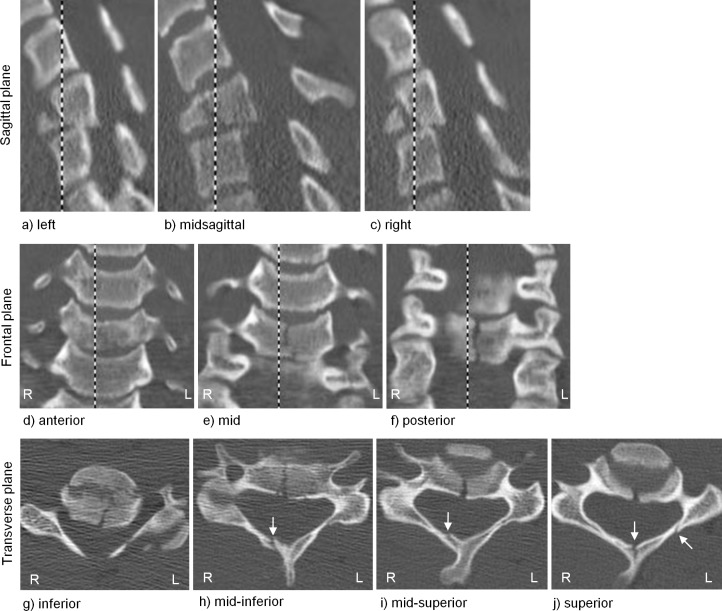
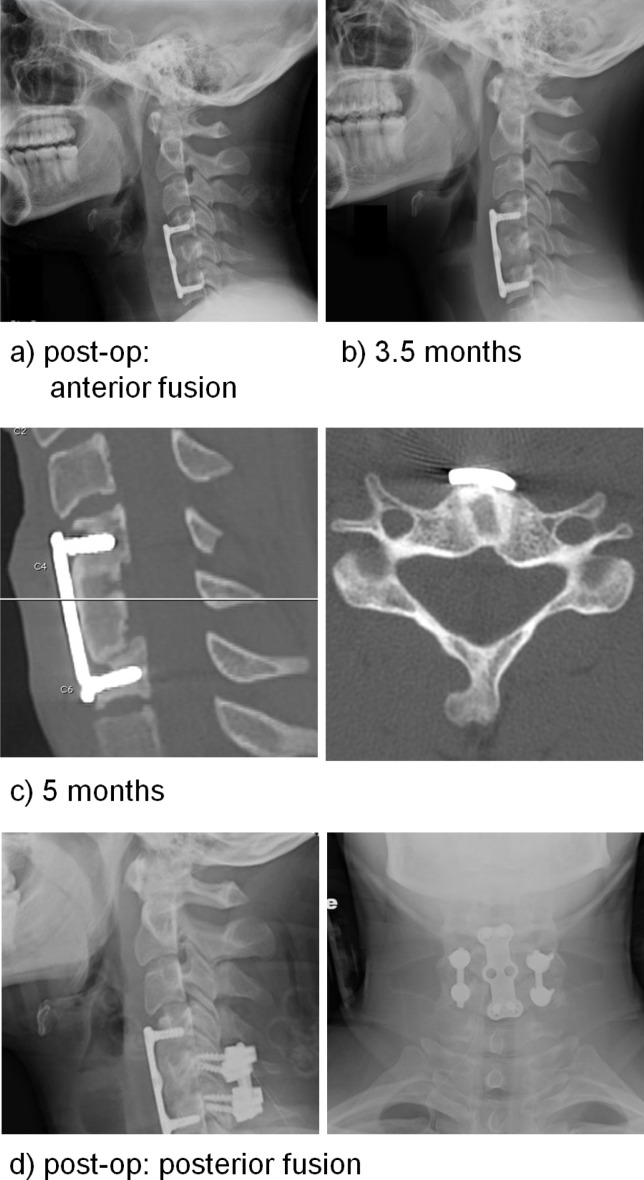
Methods: Admission imaging revealed the teardrop fracture which consisted of: a frontal plane fracture which separated an anterior quadrilateral-shaped fragment from the posterior vertebral body; a vertical fracture of the posterior vertebral body in the sagittal plane; and incomplete fractures of the neural arch that initiated superiorly at the anterior aspect of the spinous process and left lamina adjacent to the superior facet. Epidural hematoma in the region of the C5 vertebra was observed in addition to disc and ligamentous disruptions at C4-5 and C5-6. Our patient was ultimately treated surgically with anterior fusion from C4 through C6 and subsequently with bilateral posterior fusion at C5-6.
Results: The injuries were caused by high-energy axial compression with the neck in a pre-flexed posture. The first fracture event consisted of the anterior vertebral body fragment being sheared off of the posterior fragment under the compression load due in part to the sagittal plane concavity of the C5 inferior endplate. The etiology of the vertical fracture of the posterior vertebral body fragment in the sagittal plane was consistent with a previously described hypothesis of the mechanistic injury events. First, the C4-5 disc height decreased under load which increased its hoop stress. Next, this increased hoop stress transferred lateral forces to the C5 uncinate processes which caused their outward expansion. Finally, the outward expansion of the uncinate processes caused the left and right sides of the vertebral body to split and spread. Evidence in support of this mechanistic event sequence was provided by the neural arch fractures which initiated superiorly, average angulation of the C5 uncinate processes, and similar well-established mechanisms causing vertical fractures at other spinal regions.
Conclusions: Our case study and analyses provide insight into the etiology of the specific teardrop fracture patterns observed clinically.
Keywords: Cervical Spine; hockey; impact biomechanics; injury mechanism; teardrop fracture.
Figures

Similar articles
-
The axial load teardrop fracture. A biomechanical, clinical and roentgenographic analysis.Am J Sports Med. 1991 Jul-Aug;19(4):355-64. doi: 10.1177/036354659101900406. Am J Sports Med. 1991. PMID: 1897649 Review.
-
Flexion teardrop fracture of the cervical spine: radiographic characteristics.AJR Am J Roentgenol. 1989 Feb;152(2):319-26. doi: 10.2214/ajr.152.2.319. AJR Am J Roentgenol. 1989. PMID: 2783508
-
Axial loading injuries to the middle cervical spine segment. An analysis and classification of twenty-five cases.Am J Sports Med. 1991 Jan-Feb;19(1):6-20. doi: 10.1177/036354659101900103. Am J Sports Med. 1991. PMID: 2008932
-
Three-column ligamentous extension injury of the thoracic spine: a case report and review of the literature.Spine (Phila Pa 1976). 2007 Dec 1;32(25):E785-8. doi: 10.1097/BRS.0b013e31815b60fd. Spine (Phila Pa 1976). 2007. PMID: 18245995 Review.
-
Posterior facet load changes in adjacent segments due to moderate and severe degeneration in C5-C6 disc: a poroelastic C3-T1 finite element model study.J Spinal Disord Tech. 2012 Jun;25(4):218-25. doi: 10.1097/BSD.0b013e3182159776. J Spinal Disord Tech. 2012. PMID: 22652989
Cited by
-
Chasing the Cup: A Comprehensive Review of Spinal Cord Injuries in Hockey.Cureus. 2022 Apr 20;14(4):e24314. doi: 10.7759/cureus.24314. eCollection 2022 Apr. Cureus. 2022. PMID: 35602828 Free PMC article. Review.
-
Cervical Spine Injuries in the Ice Hockey Player: Current Concepts in Epidemiology, Management and Prevention.Global Spine J. 2021 Oct;11(8):1299-1306. doi: 10.1177/2192568220970549. Epub 2020 Nov 18. Global Spine J. 2021. PMID: 33203240 Free PMC article.
References
-
- Harris JH., Jr Acute injuries of the spine. Semin Roentgenol. 1978;13:53–68. - PubMed
-
- Torg JS, Pavlov H, O'Neill MJ, et al. The axial load teardrop fracture. A biomechanical, clinical and roentgenographic analysis. Am J Sports Med. 1991;19:355–64. - PubMed
-
- Richman S, Friedman RL. Vertical fracture of cervical vertebral bodies. Radiology. 1954;62:536–43. - PubMed
-
- Lee C, Kim KS, Rogers LF. Triangular cervical vertebral body fractures: diagnostic significance. AJR Am J Roentgenol. 1982;138:1123–32. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous