

Smoking Behavior and Healthcare Expenditure in the United States, 1992-2009: Panel Data Estimates
- PMID: 27163933
- PMCID: PMC4862673
- DOI: 10.1371/journal.pmed.1002020
Smoking Behavior and Healthcare Expenditure in the United States, 1992-2009: Panel Data Estimates
Erratum in
-
Correction: Smoking Behavior and Healthcare Expenditure in the United States, 1992-2009: Panel Data Estimates.PLoS Med. 2016 Jun 15;13(6):e1002070. doi: 10.1371/journal.pmed.1002070. eCollection 2016 Jun. PLoS Med. 2016. PMID: 27305149 Free PMC article.
Abstract
Background: Reductions in smoking in Arizona and California have been shown to be associated with reduced per capita healthcare expenditures in these states compared to control populations in the rest of the US. This paper extends that analysis to all states and estimates changes in healthcare expenditure attributable to changes in aggregate measures of smoking behavior in all states.
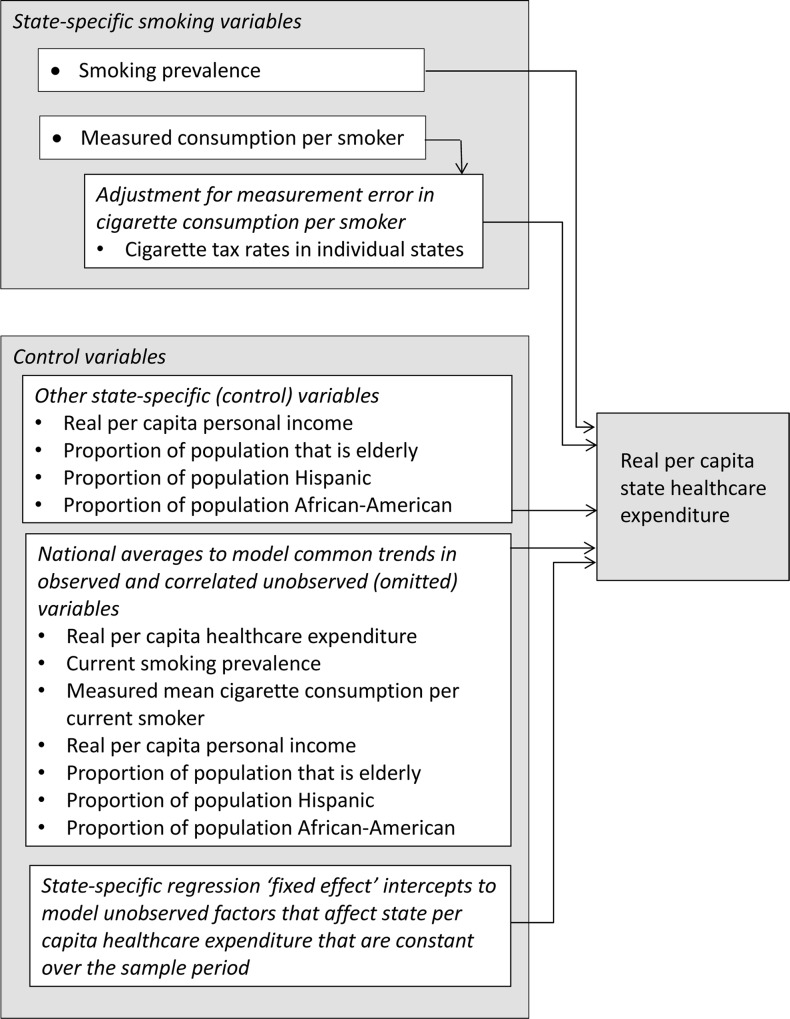
Methods and findings: State per capita healthcare expenditure is modeled as a function of current smoking prevalence, mean cigarette consumption per smoker, other demographic and economic factors, and cross-sectional time trends using a fixed effects panel data regression on annual time series data for each the 50 states and the District of Columbia for the years 1992 through 2009. We found that 1% relative reductions in current smoking prevalence and mean packs smoked per current smoker are associated with 0.118% (standard error [SE] 0.0259%, p < 0.001) and 0.108% (SE 0.0253%, p < 0.001) reductions in per capita healthcare expenditure (elasticities). The results of this study are subject to the limitations of analysis of aggregate observational data, particularly that a study of this nature that uses aggregate data and a relatively small sample size cannot, by itself, establish a causal connection between smoking behavior and healthcare costs. Historical regional variations in smoking behavior (including those due to the effects of state tobacco control programs, smoking restrictions, and differences in taxation) are associated with substantial differences in per capita healthcare expenditures across the United States. Those regions (and the states in them) that have lower smoking have substantially lower medical costs. Likewise, those that have higher smoking have higher medical costs. Sensitivity analysis confirmed that these results are robust.
Conclusions: Changes in healthcare expenditure appear quickly after changes in smoking behavior. A 10% relative drop in smoking in every state is predicted to be followed by an expected $63 billion reduction (in 2012 US dollars) in healthcare expenditure the next year. State and national policies that reduce smoking should be part of short term healthcare cost containment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
How Much Can the USA Reduce Health Care Costs by Reducing Smoking?PLoS Med. 2016 May 10;13(5):e1002021. doi: 10.1371/journal.pmed.1002021. eCollection 2016 May. PLoS Med. 2016. PMID: 27164007 Free PMC article.
Similar articles
-
The effect of the California tobacco control program on smoking prevalence, cigarette consumption, and healthcare costs: 1989-2008.PLoS One. 2013;8(2):e47145. doi: 10.1371/journal.pone.0047145. Epub 2013 Feb 13. PLoS One. 2013. PMID: 23418411 Free PMC article.
-
Predictive validation and forecasts of short-term changes in healthcare expenditure associated with changes in smoking behavior in the United States.PLoS One. 2020 Jan 16;15(1):e0227493. doi: 10.1371/journal.pone.0227493. eCollection 2020. PLoS One. 2020. PMID: 31945079 Free PMC article.
-
Smoking and healthcare expenditure reductions associated with the California Tobacco Control Program, 1989 to 2019: A predictive validation.PLoS One. 2023 Mar 16;18(3):e0263579. doi: 10.1371/journal.pone.0263579. eCollection 2023. PLoS One. 2023. PMID: 36928830 Free PMC article.
-
The Economic Impact of Smoking and of Reducing Smoking Prevalence: Review of Evidence.Tob Use Insights. 2015 Jul 14;8:1-35. doi: 10.4137/TUI.S15628. eCollection 2015. Tob Use Insights. 2015. PMID: 26242225 Free PMC article. Review.
-
Medical costs of smoking in the United States: estimates, their validity, and their implications.Tob Control. 1999 Autumn;8(3):290-300. doi: 10.1136/tc.8.3.290. Tob Control. 1999. PMID: 10599574 Free PMC article. Review.
Cited by
-
Examining the Association between Abstinence from Smoking and Healthcare Costs among Patients with Cancer.Cancer Prev Res (Phila). 2024 May 2;17(5):217-225. doi: 10.1158/1940-6207.CAPR-23-0245. Cancer Prev Res (Phila). 2024. PMID: 37940143 Free PMC article.
-
Association between smoking cessation and post-hospitalization healthcare costs: a matched cohort analysis.BMC Health Serv Res. 2019 Dec 2;19(1):924. doi: 10.1186/s12913-019-4777-7. BMC Health Serv Res. 2019. PMID: 31791307 Free PMC article. Clinical Trial.
-
The experimental tobacco marketplace: Narrative influence on electronic cigarette substitution.Exp Clin Psychopharmacol. 2019 Apr;27(2):115-124. doi: 10.1037/pha0000233. Epub 2018 Nov 5. Exp Clin Psychopharmacol. 2019. PMID: 30394764 Free PMC article.
-
Racial and Income Disparities in Health-Related Quality of Life among Smokers with a Quit Attempt in Louisiana.Medicina (Kaunas). 2019 Feb 13;55(2):48. doi: 10.3390/medicina55020048. Medicina (Kaunas). 2019. PMID: 30781893 Free PMC article.
-
The Economics of Tobacco Regulation: A Comprehensive Review.J Econ Lit. 2022 Sep;60(3):883-970. doi: 10.1257/jel.20201482. J Econ Lit. 2022. PMID: 37075070 Free PMC article.
References
-
- US Department of Health and Human Services (2014) The health consequences of smoking—50 years of progress: a report of the Surgeon General Rockville (Maryland): US Department of Health and Human Services.
-
- Lightwood JM, Glantz SA (1997) Short-term economic and health benefits of smoking cessation: myocardial infarction and stroke. Circulation 96: 1089–1096. - PubMed
-
- Lightwood JM, Phibbs CS, Glantz SA (1999) Short-term health and economic benefits of smoking cessation: low birth weight. Pediatrics 104: 1312–1320. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
