

The vascular anatomy of the ligaments of the liver: gross anatomy, imaging and clinical applications
- PMID: 27163944
- PMCID: PMC5124872
- DOI: 10.1259/bjr.20150925
The vascular anatomy of the ligaments of the liver: gross anatomy, imaging and clinical applications
Abstract
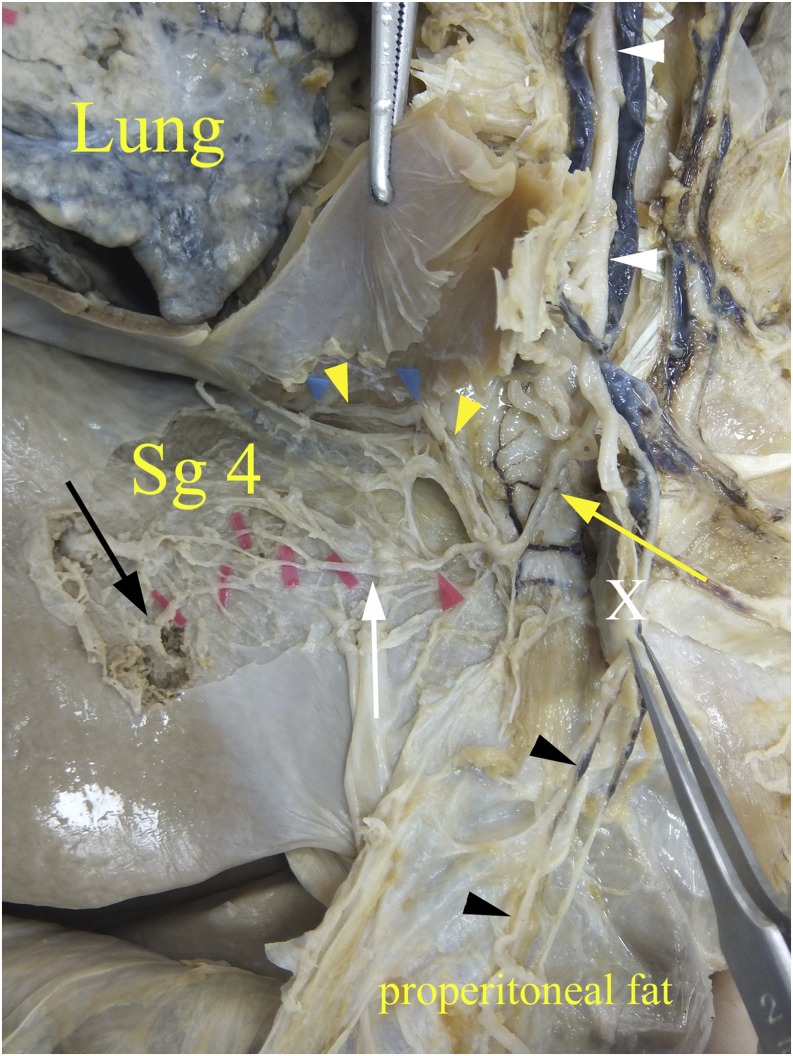
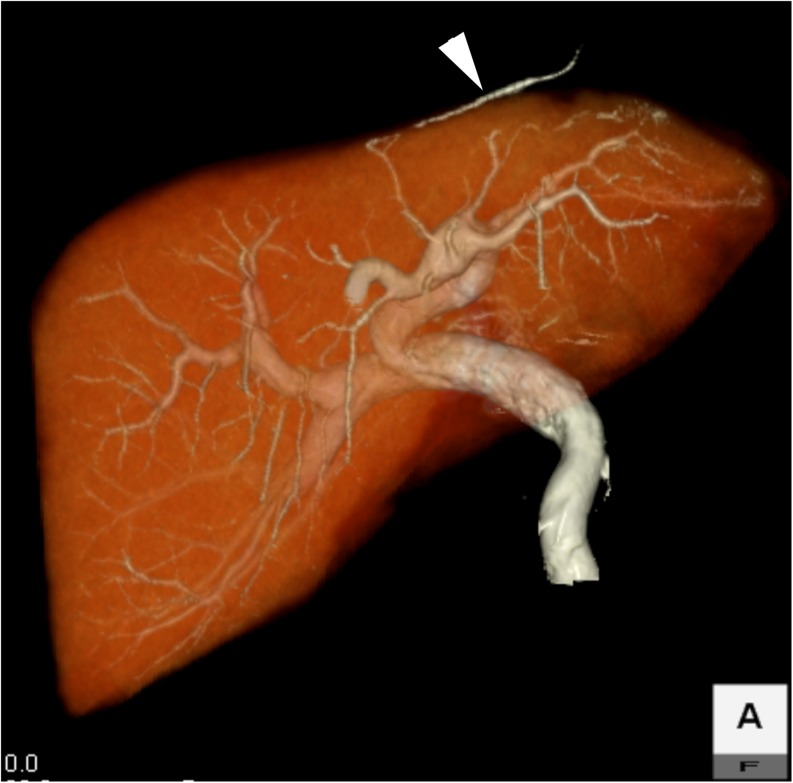
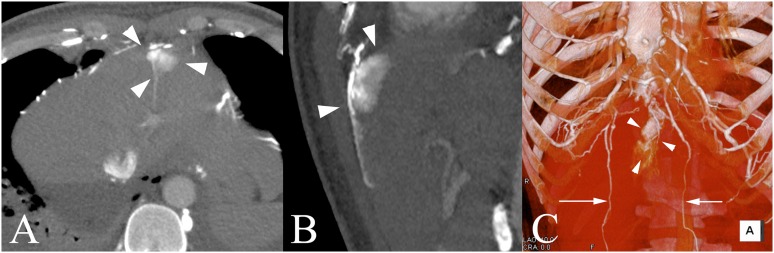
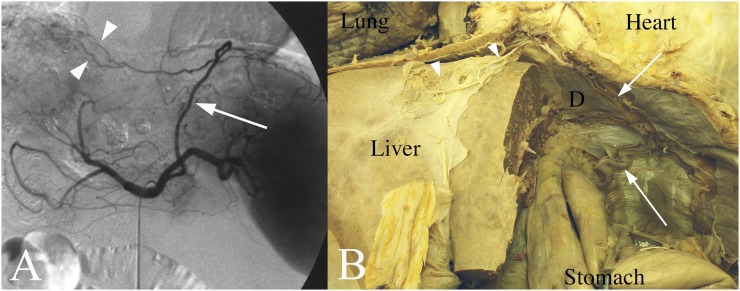
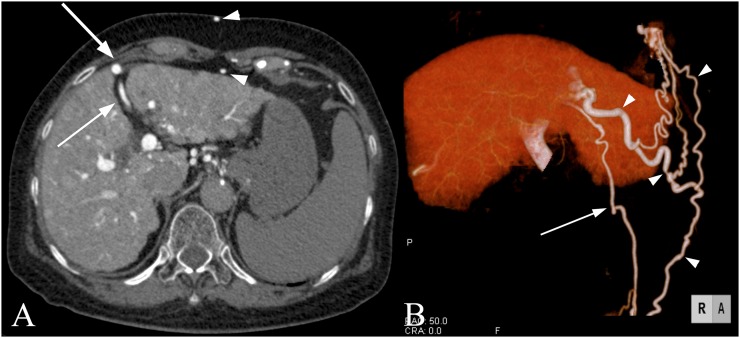
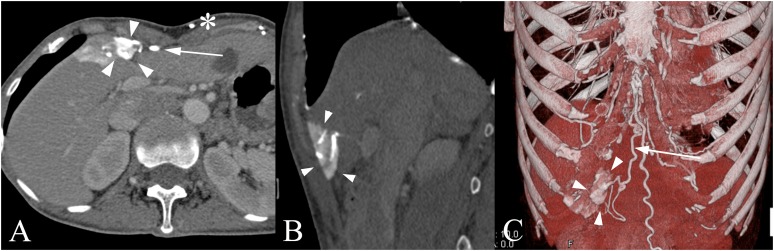
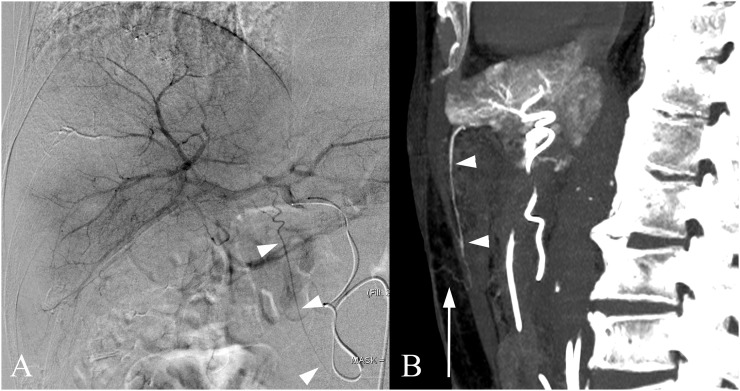
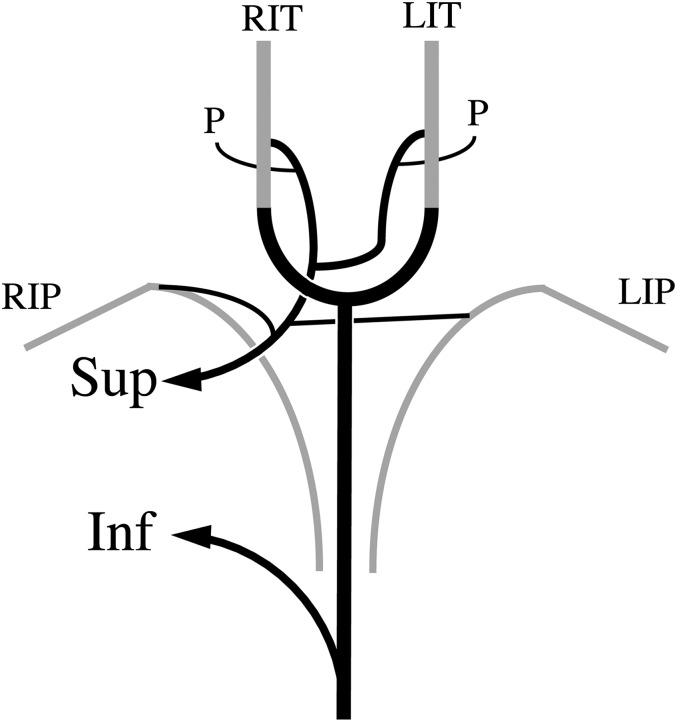
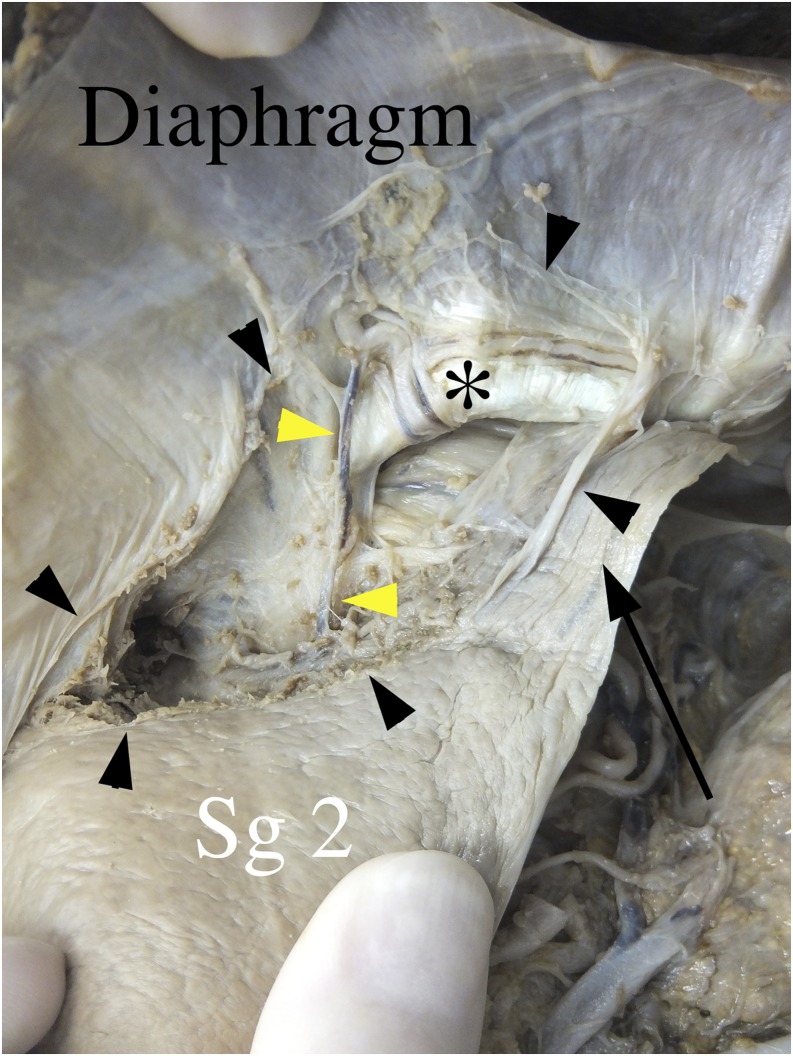
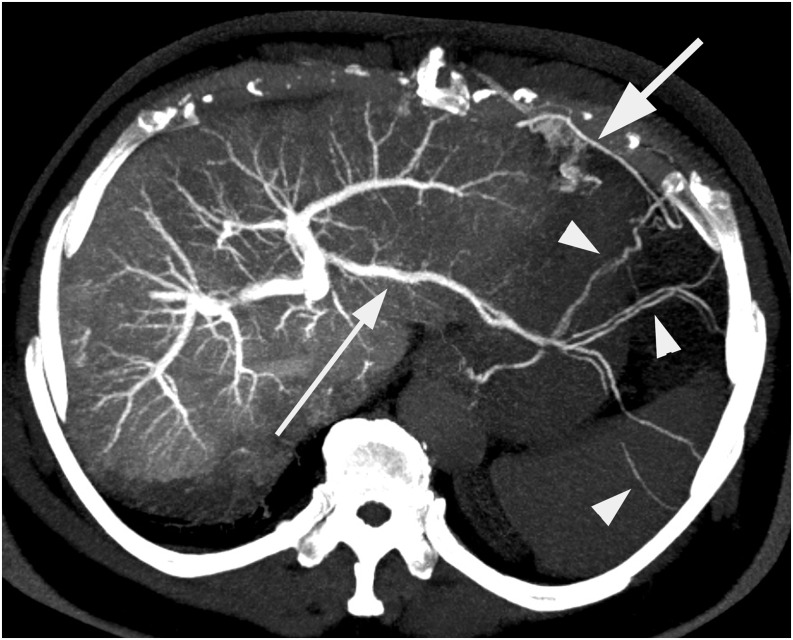
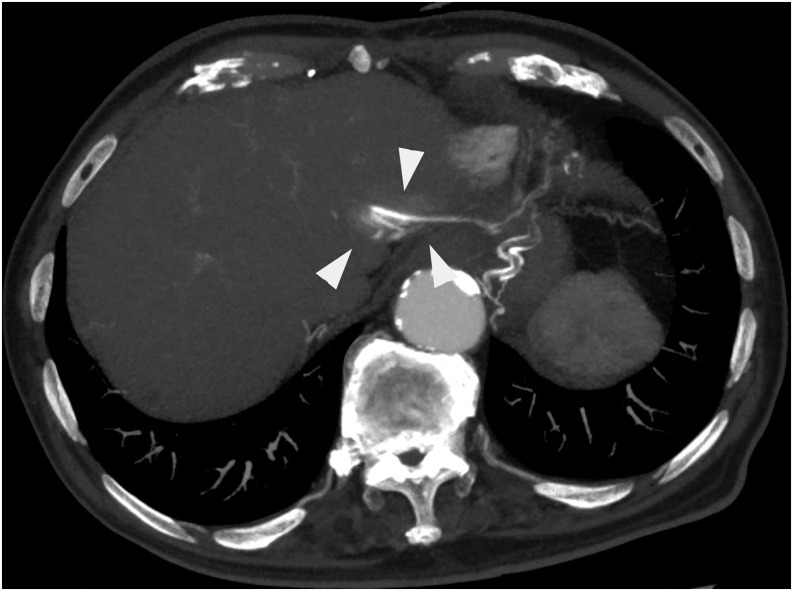
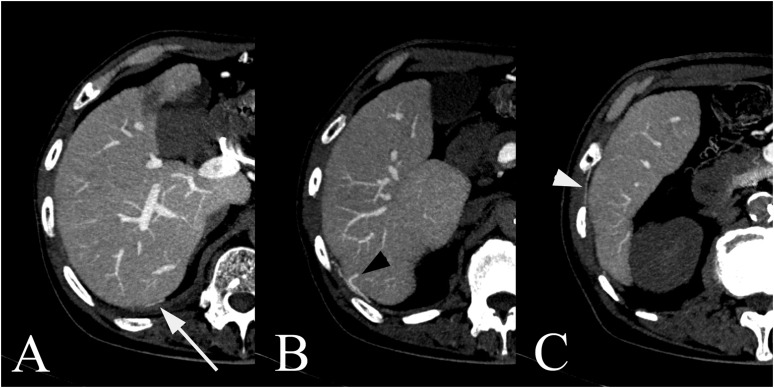
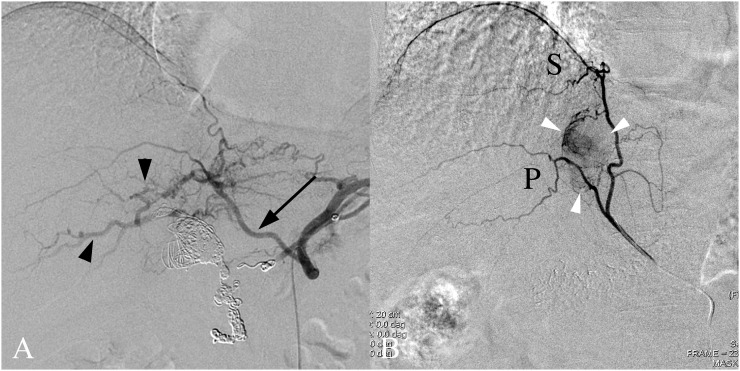
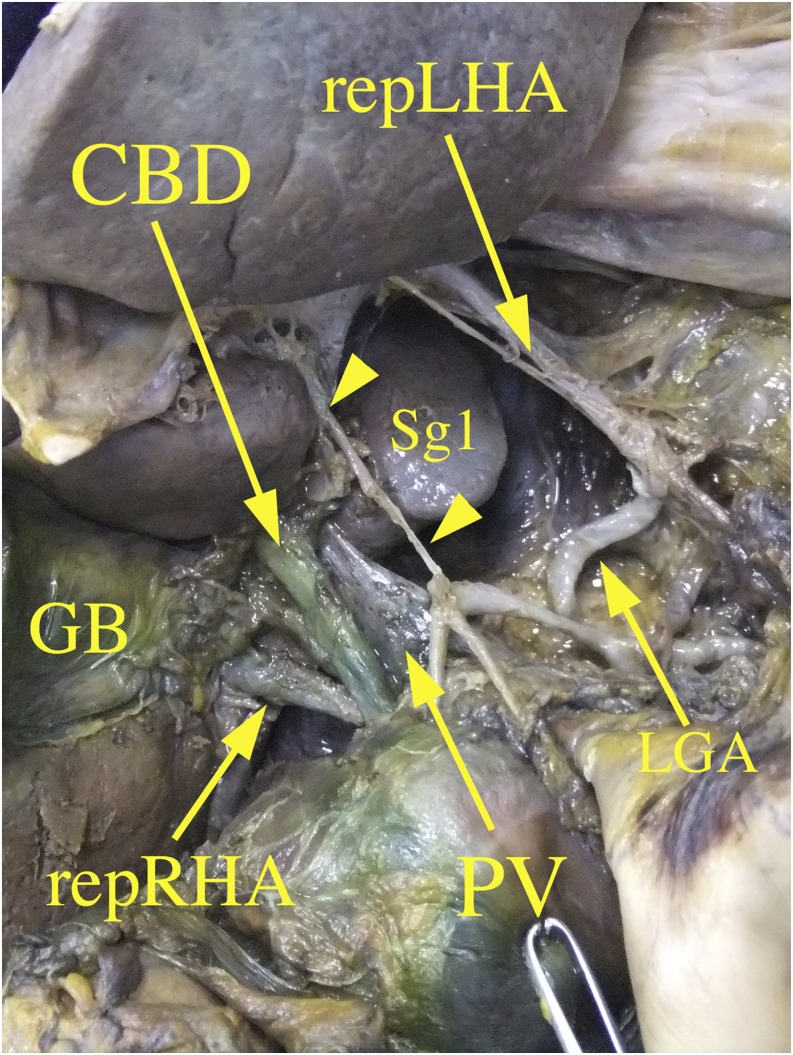
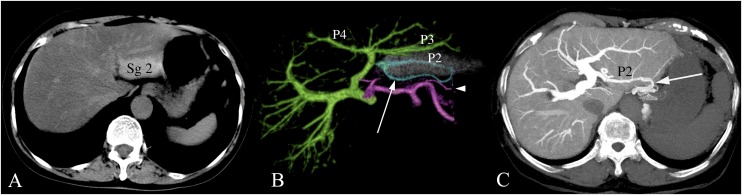
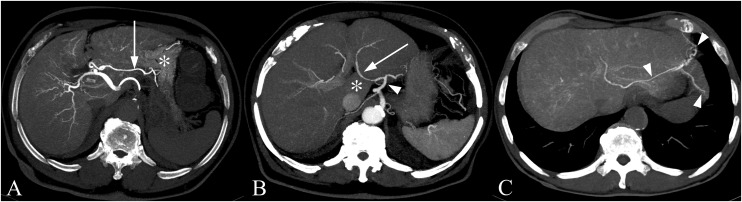
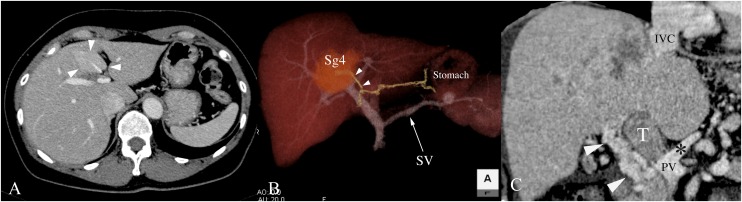
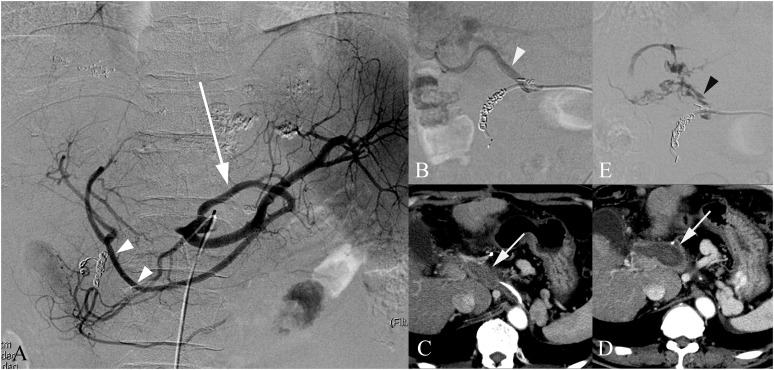
The vessels that communicate between the liver and adjacent structures require bridges between them. The bridges comprise the ligaments of the liver as follows: the falciform ligament, right and left coronary ligaments, lesser omentum including the hepatogastric ligament and hepatoduodenal ligament. Each ligament has specific communications between the intrahepatic and extrahapetic vessels. The venous communications called as the portosystemic shunt would become apparent in patients with portal hypertension, intrahepatic portal vein thrombosis and superior vena cava syndrome. The location of the venous communication is related to the pseudolesion or focal enhancement of the liver demonstrated on the CT scan. The arterial communications called collateral vascularization would become apparent in patients with hepatic artery occlusion, especially post-transhepatic arterial embolization, or in patients with the hepatic tumour abutting diaphragm. The knowledge of these collateral arteries is necessary to accomplish the effective transarterial embolization for the hepatic tumours. We reviewed the vessels in these ligaments using contrast-enhanced CT scans and angiography and discussed the clinical applications. Cadaver dissection photos were included as supplementary images for readers to recognize the actual spatial anatomy of the vessel in each ligament.
Figures
Similar articles
-
Pseudolesions of left liver lobe during helical CT examinations: prevalence and comparison between unenhanced and biphasic CT findings.Eur J Radiol. 2005 Jun;54(3):388-92. doi: 10.1016/j.ejrad.2004.07.016. Eur J Radiol. 2005. PMID: 15899341
-
[Study of the liver and the portal venous system with digital rotational angiography].Radiol Med. 2001 Mar;101(3):118-24. Radiol Med. 2001. PMID: 11402948 Italian.
-
Symptomatic intrahepatic portosystemic venous shunt: embolization with an alternative approach.AJR Am J Roentgenol. 2003 Jul;181(1):71-8. doi: 10.2214/ajr.181.1.1810071. AJR Am J Roentgenol. 2003. PMID: 12818832
-
The hepatic capsular arteries: imaging features and clinical significance.Abdom Radiol (NY). 2019 Aug;44(8):2729-2739. doi: 10.1007/s00261-019-02021-3. Abdom Radiol (NY). 2019. PMID: 31028433 Review.
-
The clinical anatomy of congenital portosystemic venous shunts.Clin Anat. 2008 Mar;21(2):147-57. doi: 10.1002/ca.20574. Clin Anat. 2008. PMID: 18161055 Review.
Cited by
-
Successful use of ligamentum teres hepatis for perforated duodenal ulcer following omentectomy: a case report.J Surg Case Rep. 2020 Jul 31;2020(7):rjaa196. doi: 10.1093/jscr/rjaa196. eCollection 2020 Jul. J Surg Case Rep. 2020. PMID: 32760488 Free PMC article.
-
Pseudolesion in the right parafissural liver parenchyma on CT: The base is found in embryology and collagen content.PLoS One. 2020 Jan 27;15(1):e0221544. doi: 10.1371/journal.pone.0221544. eCollection 2020. PLoS One. 2020. PMID: 31986149 Free PMC article.
-
Laparoscopic left hepatectomy for a patient with intrahepatic cholangiocarcinoma metastasis in the falciform ligament: a case report.BMC Surg. 2021 Mar 8;21(1):122. doi: 10.1186/s12893-021-01115-4. BMC Surg. 2021. PMID: 33685435 Free PMC article.
-
Left Hemi-Hepatectomy to Resect Metastatic Tumor of Round Ligament of Liver in Patients with Ovarian Cancer.Cancers (Basel). 2024 Aug 30;16(17):3036. doi: 10.3390/cancers16173036. Cancers (Basel). 2024. PMID: 39272893 Free PMC article.
-
Umbilical cord vessels other than the umbilical arteries and vein: a histological study of midterm human fetuses.Anat Cell Biol. 2022 Dec 31;55(4):467-474. doi: 10.5115/acb.22.102. Epub 2022 Oct 19. Anat Cell Biol. 2022. PMID: 36258268 Free PMC article.
References
-
- Warwick R, Williams PL, eds. Gray's anatomy. 35th edn. London, UK: Longmans; 1973. p. 178.
-
- Arey LB. Developmental Anatomy. 6th edn. Tokyo, Japan: Charles E. Tuttle Co.; 1966. pp. 279–80.
-
- Sappey MC. Thesis on the accessory portal veins. [In French.] Journal de l'anatomie et de la physiologie normales et pathologiques de l'homme et des animaux 1883; 19: 517–25.
LinkOut - more resources
Full Text Sources
Other Literature Sources
