

Human Myeloid-derived Suppressor Cells are Associated With Chronic Immune Suppression After Severe Sepsis/Septic Shock
- PMID: 27163951
- PMCID: PMC5102824
- DOI: 10.1097/SLA.0000000000001783
Human Myeloid-derived Suppressor Cells are Associated With Chronic Immune Suppression After Severe Sepsis/Septic Shock
Abstract
Objective: We hypothesized that after sepsis in humans, MDSCs will be persistently increased, functionally immunosuppressive, and associated with adverse clinical outcomes.
Background: Cancer and sepsis have surprisingly similar immunologic responses and equally dismal long term consequences. In cancer, increased myeloid-derived suppressor cells (MDSCs) induce detrimental immunosuppression, but little is known about the role of MDSCs after sepsis.
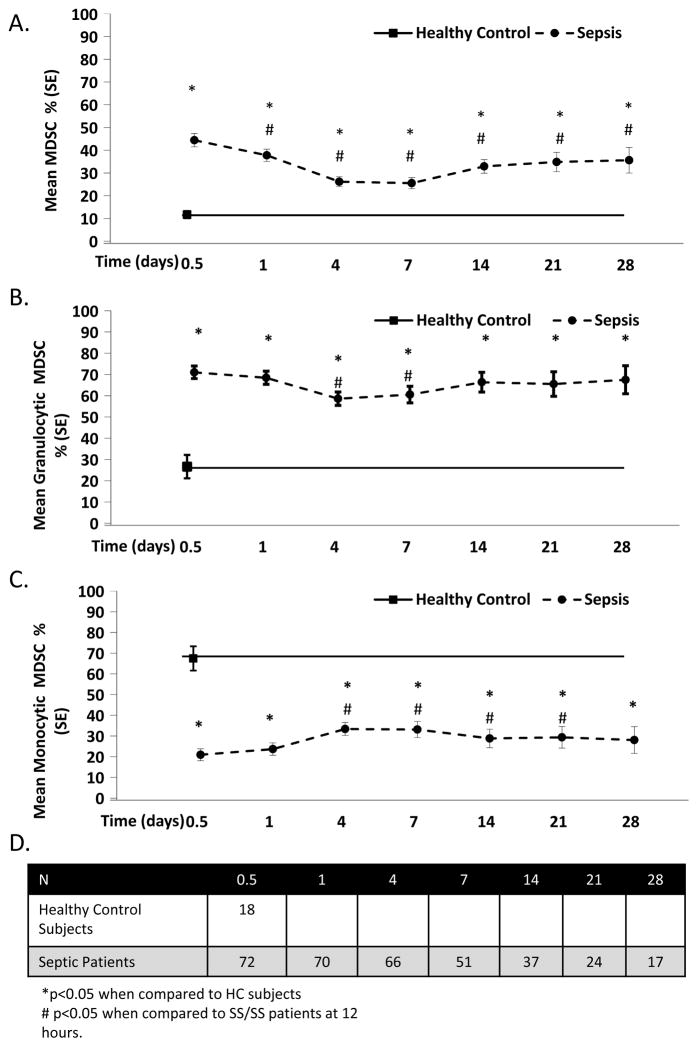
Methods: Blood was obtained from 74 patients within 12 hours of severe sepsis/septic shock (SS/SS), and at set intervals out to 28 days, and also in 18 healthy controls. MDSCs were phenotyped for cell surface receptor expression and enriched by cell sorting. Functional and genome-wide expression analyses were performed. Multiple logistic regression analysis was conducted to determine if increased MDSC appearance was associated with in-hospital and long-term outcomes.
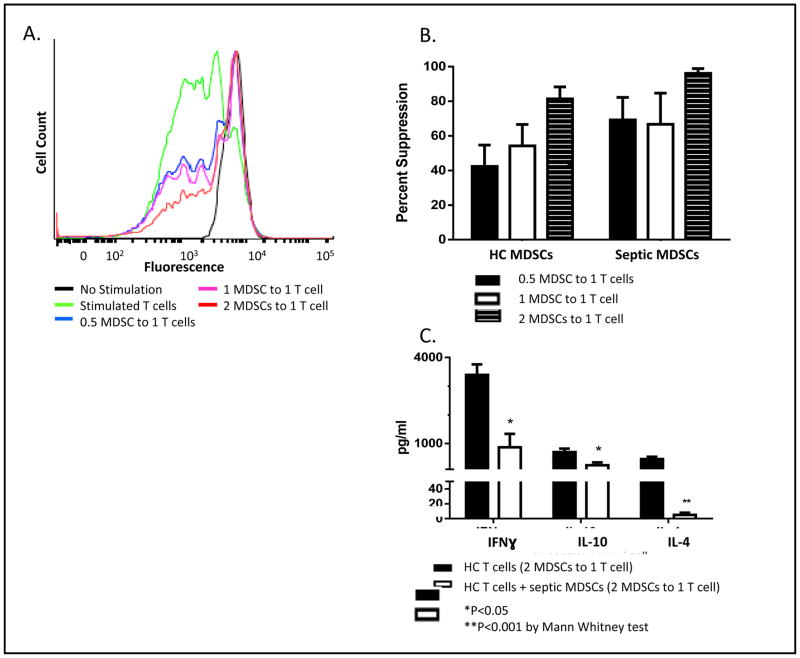
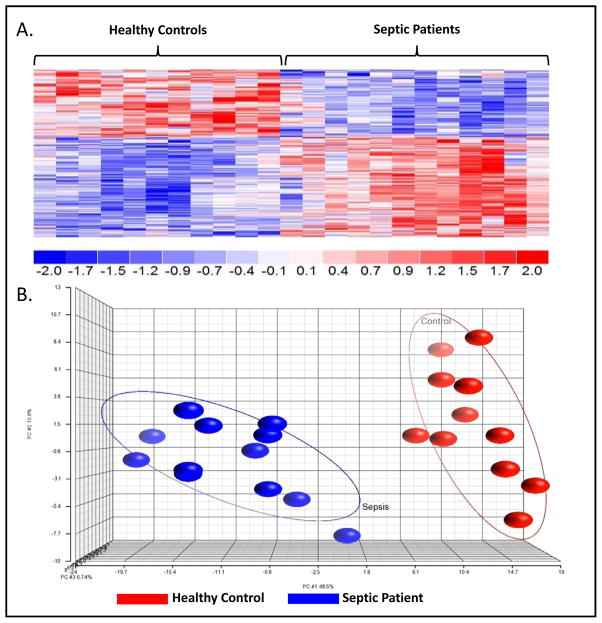
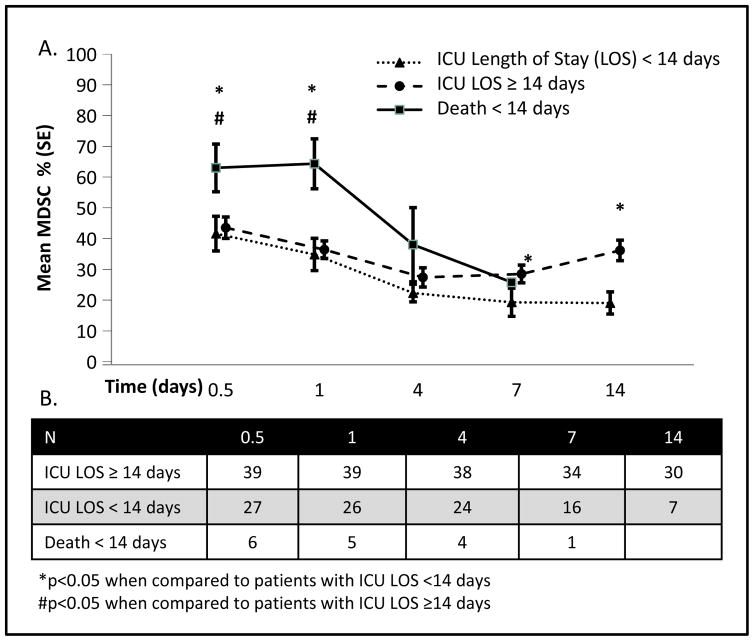
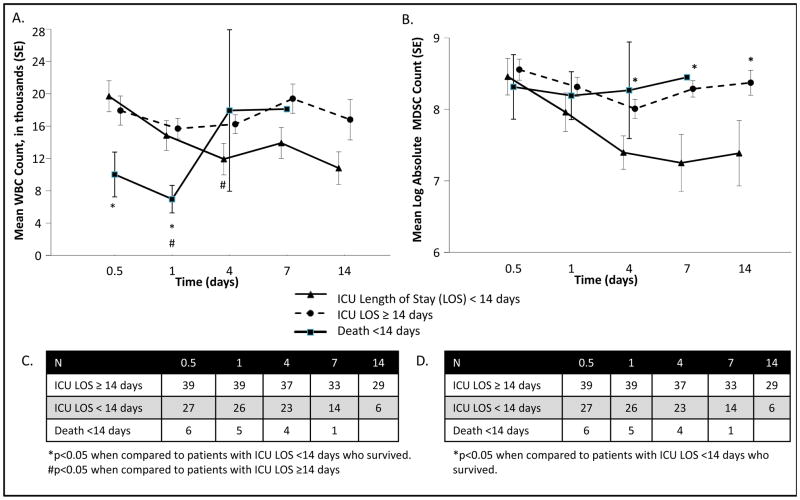
Results: After SS/SS, CD33CD11bHLA-DR MDSCs were dramatically increased out to 28 days (P < 0.05). When co-cultured with MDSCs from SS/SS patients, antigen-driven T-cell proliferation and TH1/TH2 cytokine production were suppressed (P < 0.05). Additionally, septic MDSCs had suppressed HLA gene expression and up-regulated ARG1 expression (P < 0.05). Finally, SS/SS patients with persistent increased percentages of blood MDSCs had increased nosocomial infections, prolonged intensive care unit stays, and poor functional status at discharge (P < 0.05).
Conclusions: After SS/SS in humans, circulating MDSCs are persistently increased, functionally immunosuppressive, and associated with adverse outcomes. This novel observation warrants further studies. As observed in cancer immunotherapy, MDSCs could be a novel component in multimodality immunotherapy targeting detrimental inflammation and immunosuppression after SS/SS to improve currently observed dismal long-term outcomes.
Conflict of interest statement
Conflict of Interest and Financial Disclosure Statement: No conflict of or competing interests have been declared.
Figures
References
-
- [Accessed Feb. 17, 2016];National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. 2011 Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.pdf. - PubMed
-
- Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. Jama. 1997;278(3):234–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
