

Multi-institutional Validation Study of the American Joint Commission on Cancer (8th Edition) Changes for T and N Staging in Patients With Pancreatic Adenocarcinoma
- PMID: 27163957
- PMCID: PMC5611666
- DOI: 10.1097/SLA.0000000000001763
Multi-institutional Validation Study of the American Joint Commission on Cancer (8th Edition) Changes for T and N Staging in Patients With Pancreatic Adenocarcinoma
Abstract
Objective: The aim of this study was to evaluate and validate the proposed 8th edition American Joint Committee on Cancer (AJCC) system for T and N staging of pancreatic adenocarcinoma.
Summary of background data: Investigators have questioned the clinical relevance and reproducibility of previous AJCC staging for pancreatic adenocarcinoma.
Methods: Prospective databases at Memorial Sloan Kettering (MSK), Massachusetts General Hospital (MGH), and Johns Hopkins Hospital (JHH) were queried for patients who had undergone resection for pancreatic adenocarcinoma. Patients who underwent a margin-negative (R0) resection, and who had previously undergone pathologic review, were included. Patients were staged according to 7th edition AJCC criteria, as well as the proposed 8th edition system that includes different definitions of tumor size (T) and nodal status (N). The dataset was randomly split into training and test sets.
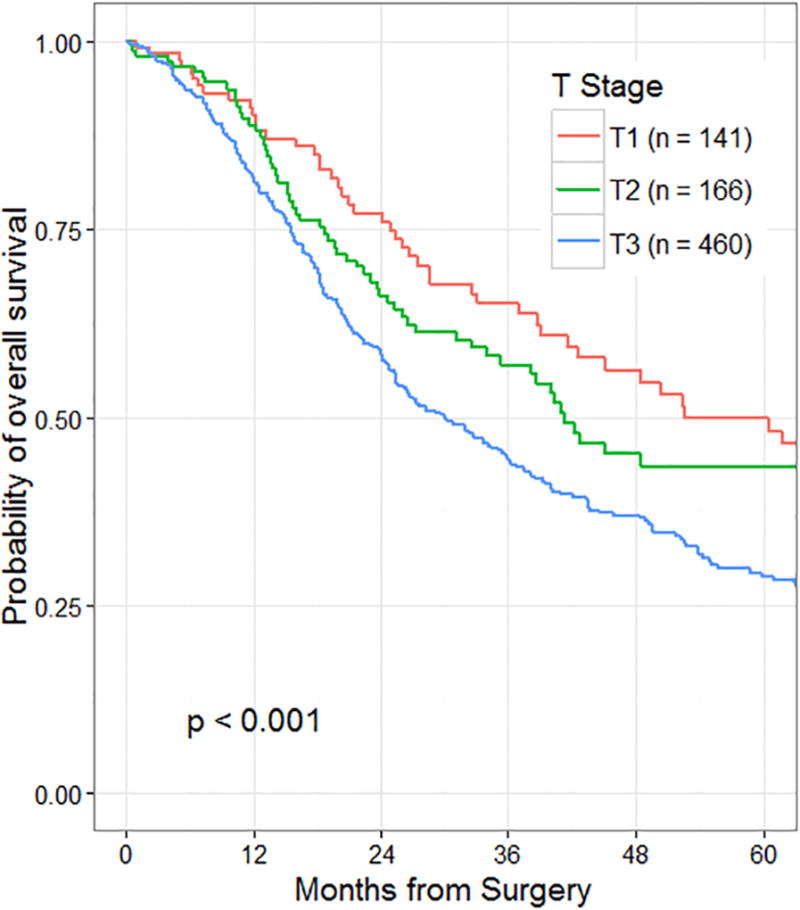
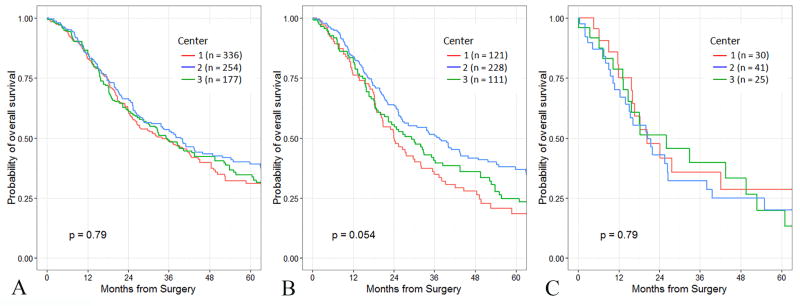
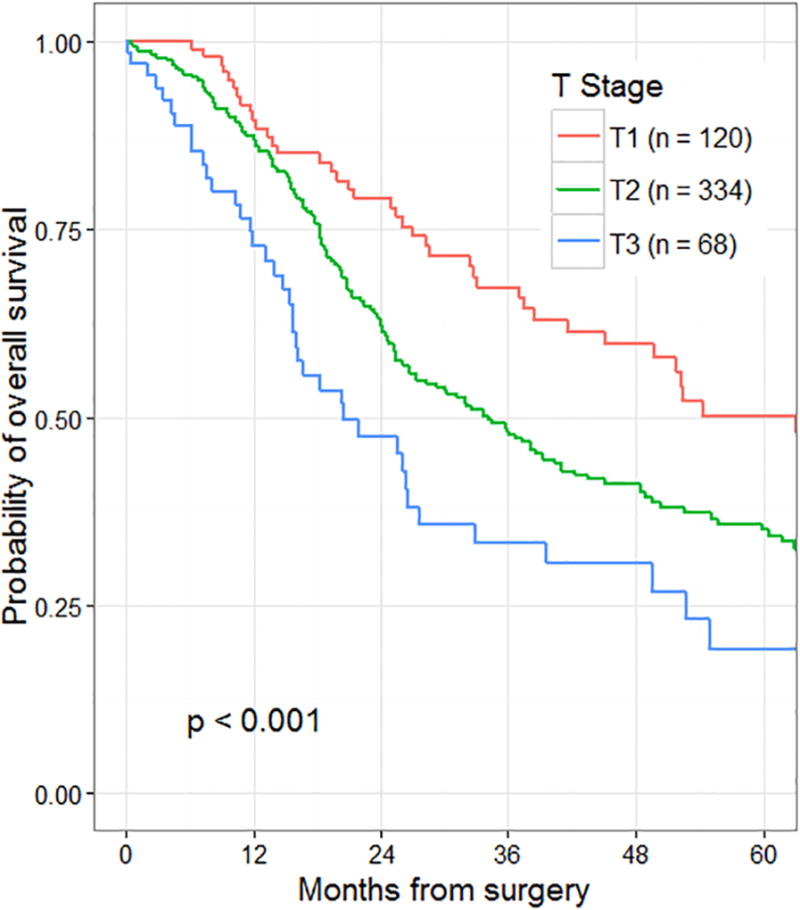
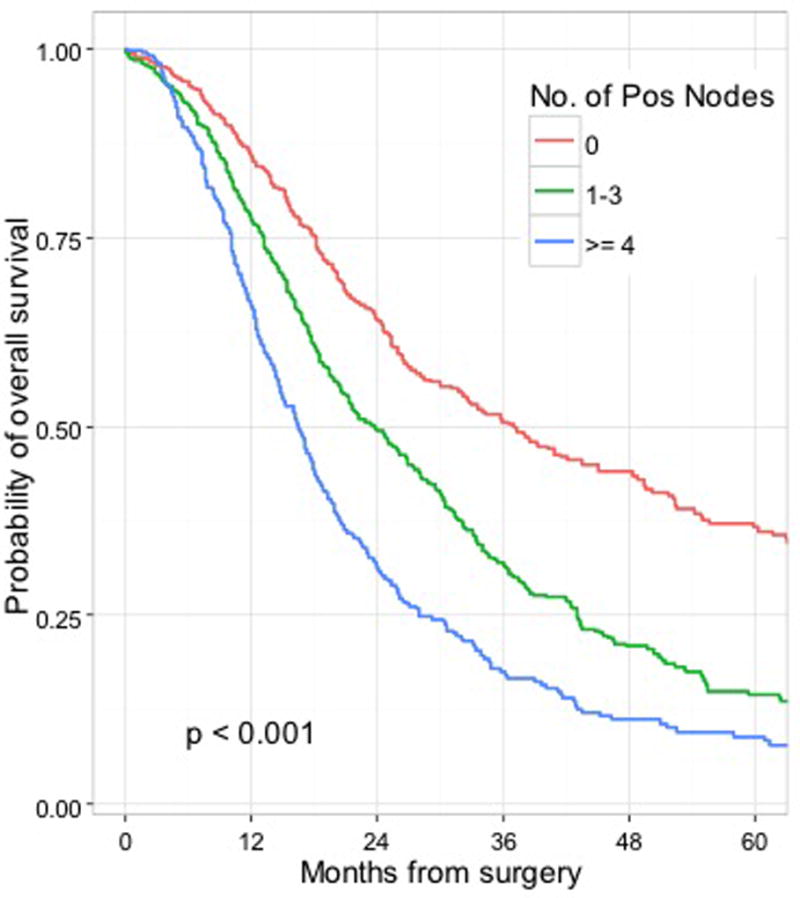
Results: Two thousand three hundred eighteen patients were identified who met inclusion criteria. Recursive partitioning on the training set (n = 1551) identified statistically appropriate cutoffs for tumor size (<2.2 cm, ≥4.8 cm,) and nodal status (no positive nodes, 1 to 3 positive nodes, ≥4 positive nodes) that supported the proposed 8th edition changes. Median survival in patients staged as T3, N0 by the 7th edition definitions was different between institutions (median Center 1, 24 mo; Center 2, 37 mo; Center 3, 29 mo; P = 0.054). This difference was not observed when patients were staged as T3, N0 by 8th edition criteria. Stage, and stage-specific outcome (7th edition), on the test set revealed a predominance of patients (68%) within the IIB subgroup, and a concordance probability estimate (CPE) of 0.57 for stage-specific survival. When assessed with 8th edition criteria, no stage subgroup had a majority of patients, and the CPE was 0.58.
Conclusions: The proposed 8th edition changes for T and N classification were statistically valid and may allow a more reproducible system of T staging. This system also stratifies patients more evenly across stages without sacrificing prognostic accuracy.
Figures
References
-
- Edge SB, Byrd DR, Compton CC, et al. AJCC Cancer Staging Manual. New York: Springer; 2010.
-
- Adsay NV, Bagci P, Tajiri T, et al. Pathologic staging of pancreatic, ampullary, biliary, and gallbladder cancers: pitfalls and practical limitations of the current AJCC/UICC TNM staging system and opportunities for improvement. Semin Diagn Pathol. 2012;29:127–141. - PubMed
-
- Strobel O, Hinz U, Gluth A, et al. Pancreatic adenocarcinoma: number of positive nodes allows to distinguish several N categories. Ann Surg. 2015;261:961–969. - PubMed
-
- Murakami Y, Uemura K, Sudo T, et al. Number of metastatic lymph nodes, but not lymph node ratio, is an independent prognostic factor after resection of pancreatic carcinoma. J Am Coll Surg. 2010;211:196–204. - PubMed
-
- Basturk O, Saka B, Balci S, et al. Substaging of Lymph Node Status in Resected Pancreatic Ductal Adenocarcinoma Has Strong Prognostic Correlations: Proposal for a Revised N Classification for TNM Staging. Ann Surg Oncol. 2015;22(Suppl 3):1187–1195. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
