

Subacute decline in serum lipids precedes the occurrence of primary intracerebral hemorrhage
- PMID: 27164693
- PMCID: PMC4891207
- DOI: 10.1212/WNL.0000000000002716
Subacute decline in serum lipids precedes the occurrence of primary intracerebral hemorrhage
Abstract
Objective: We aimed to describe the temporal variation in circulating lipid levels among patients with intracerebral hemorrhage (ICH) and investigate their association with ICH risk.
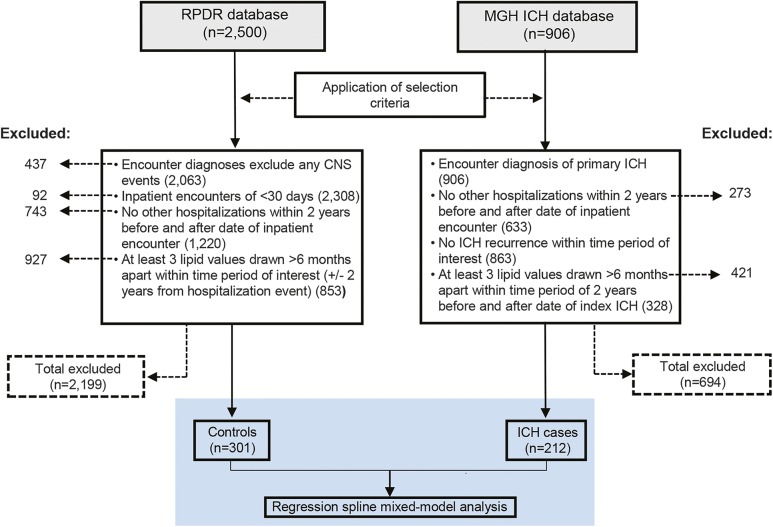
Methods: This was a single-center, retrospective, longitudinal, case-control analysis using cases drawn from an ongoing cohort study of primary ICH and controls drawn from a hospital-based clinical data registry. Piecewise linear mixed-effect random coefficient models were used to determine the significance of changes in serum lipid trends on ICH risk.
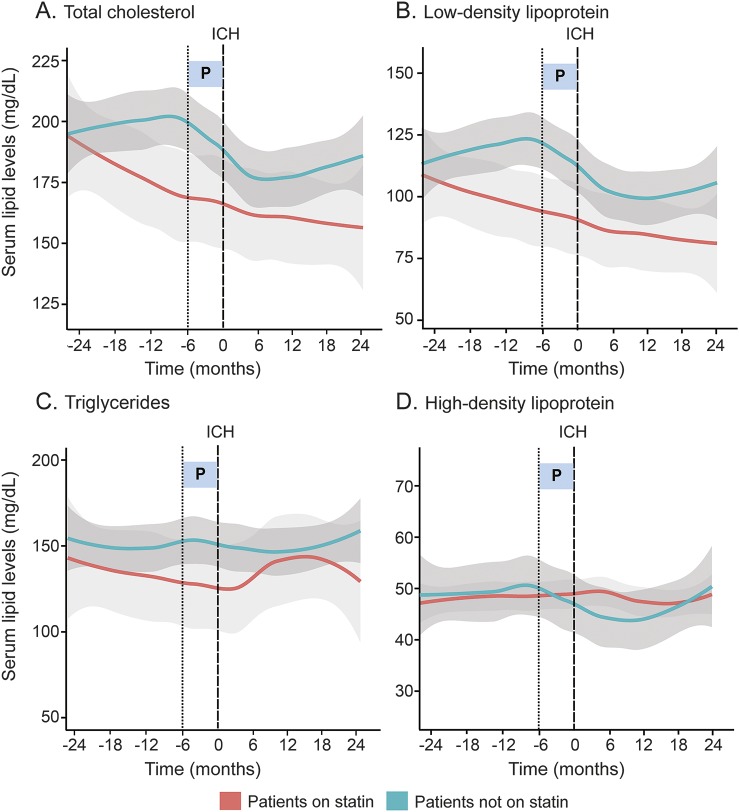
Results: Two hundred twelve ICH cases and 301 control individuals were analyzed. Overall trends in serum total cholesterol (TC) and low-density lipoprotein (LDL) levels differed between ICH cases and non-ICH controls (p = 0.00001 and p = 0.0092, respectively). Patients with ICH experience accelerated decline in serum TC and LDL levels during 6 months immediately preceding ICH, compared with levels between 6 and 24 months pre-ICH (TC: -29.25 mg/dL, p = 0.001; LDL: -21.48 mg/dL, p = 0.0038), which was not observed in non-ICH controls. Subgroup analysis confirmed that this phenomenon cannot be attributed to statin or alcohol exposure. Serum triglycerides and high-density lipoprotein trends did not differ between groups.
Conclusions: Longitudinal lipid levels differ between ICH cases and non-ICH controls, most notably for a decline in serum TC and LDL levels within 6 months preceding primary ICH, independent of statin or alcohol use. These changes in serum TC and LDL trends suggest a biological pathway that precipitates ICH occurrence. Further studies are needed to replicate these results and characterize rate of change in serum lipids as a potential biomarker of impending acute cerebral injury.
© 2016 American Academy of Neurology.
Figures

Comment in
-
Lipid levels: A novel biomarker of impending intracerebral hemorrhage?Neurology. 2016 May 31;86(22):2028-9. doi: 10.1212/WNL.0000000000002726. Epub 2016 Apr 29. Neurology. 2016. PMID: 27164699 No abstract available.
References
-
- Kuller L, Reisler DM. An explanation for variations in distribution of stroke and arteriosclerotic heart disease among populations and racial groups. Am J Epidemiol 1971;93:1–9. - PubMed
-
- Yano K, Reed DM, MacLean CJ. Serum cholesterol and hemorrhagic stroke in the Honolulu Heart Program. Stroke 1989;20:1460–1465. - PubMed
-
- Iso H, Jacobs DR, Jr, Wentworth D, Neaton JD, Cohen JD. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the Multiple Risk Factor Intervention Trial. N Engl J Med 1989;320:904–910. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical