

9th Hatter Biannual Meeting: position document on ischaemia/reperfusion injury, conditioning and the ten commandments of cardioprotection
- PMID: 27164905
- PMCID: PMC4863033
- DOI: 10.1007/s00395-016-0558-1
9th Hatter Biannual Meeting: position document on ischaemia/reperfusion injury, conditioning and the ten commandments of cardioprotection
Abstract
In the 30 years since the original description of ischaemic preconditioning, understanding of the pathophysiology of ischaemia/reperfusion injury and concepts of cardioprotection have been revolutionised. In the same period of time, management of patients with coronary artery disease has also been transformed: coronary artery and valve surgery are now deemed routine with generally excellent outcomes, and the management of acute coronary syndromes has seen decade on decade reductions in cardiovascular mortality. Nonetheless, despite these improvements, cardiovascular disease and ischaemic heart disease in particular, remain the leading cause of death and a significant cause of long-term morbidity (with a concomitant increase in the incidence of heart failure) worldwide. The need for effective cardioprotective strategies has never been so pressing. However, despite unequivocal evidence of the existence of ischaemia/reperfusion in animal models providing a robust rationale for study in man, recent phase 3 clinical trials studying a variety of cardioprotective strategies in cardiac surgery and acute ST-elevation myocardial infarction have provided mixed results. The investigators meeting at the Hatter Cardiovascular Institute workshop describe the challenge of translating strong pre-clinical data into effective clinical intervention strategies in patients in whom effective medical therapy is already altering the pathophysiology of ischaemia/reperfusion injury-and lay out a clearly defined framework for future basic and clinical research to improve the chances of successful translation of strong pre-clinical interventions in man.
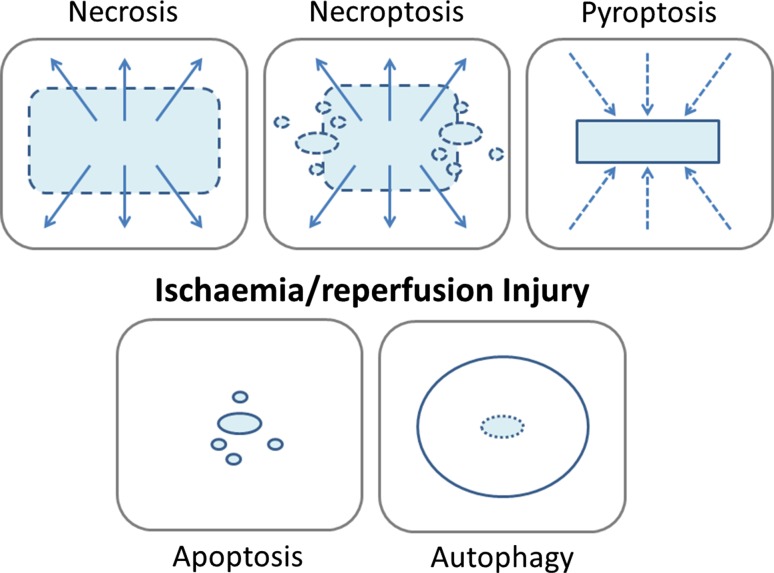
Keywords: Apoptosis; Asprin; Autophagy; Basic research; Beta blockers; CABG; Cardiac surgery; Clinical trials; Conditioning; Cyclosporine; DNA; Infarction; Injury; Ischaemia; Ischaemic; Metoprolol; Mitochondrial transition pore; Necroptosis; Necrosis; Opiates; Postconditioning; Pre-clinical; Preconditioning; Pyroptosis; RISK pathway; Reperfusion; SAFE pathway; Statins; Valve replacement; p2y12.
Figures

References
-
- Balteau M, Tajeddine N, de Meester C, Ginion A, Des Rosiers C, Brady NR, Sommereyns C, Horman S, Vanoverschelde JL, Gailly P, Hue L, Bertrand L, Beauloye C. NADPH oxidase activation by hyperglycaemia in cardiomyocytes is independent of glucose metabolism but requires SGLT1. Cardiovasc Res. 2011;92:237–246. doi: 10.1093/cvr/cvr230. - DOI - PubMed
-
- Barrabes JA, Inserte J, Mirabet M, Quiroga A, Hernando V, Figueras J, Garcia-Dorado D. Antagonism of P2Y12 or GPIIb/IIIa receptors reduces platelet-mediated myocardial injury after ischaemia and reperfusion in isolated rat hearts. Thromb Haemost. 2010;104:128–135. doi: 10.1160/TH09-07-0440. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
