

MRI in multiple myeloma: a pictorial review of diagnostic and post-treatment findings
- PMID: 27164915
- PMCID: PMC4956620
- DOI: 10.1007/s13244-016-0492-7
MRI in multiple myeloma: a pictorial review of diagnostic and post-treatment findings
Abstract
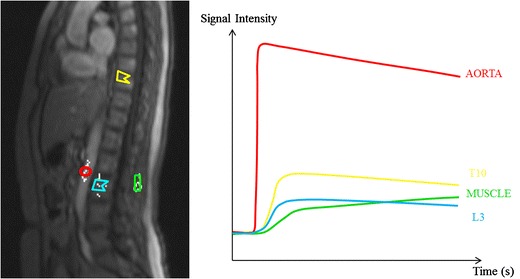
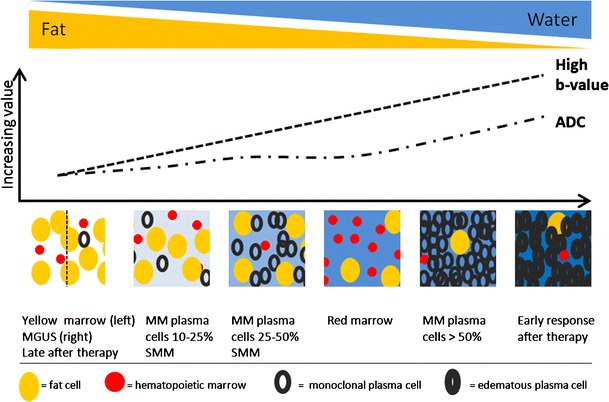
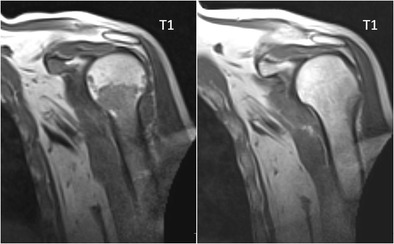
Magnetic resonance imaging (MRI) is increasingly being used in the diagnostic work-up of patients with multiple myeloma. Since 2014, MRI findings are included in the new diagnostic criteria proposed by the International Myeloma Working Group. Patients with smouldering myeloma presenting with more than one unequivocal focal lesion in the bone marrow on MRI are considered having symptomatic myeloma requiring treatment, regardless of the presence of lytic bone lesions. However, bone marrow evaluation with MRI offers more than only morphological information regarding the detection of focal lesions in patients with MM. The overall performance of MRI is enhanced by applying dynamic contrast-enhanced MRI and diffusion weighted imaging sequences, providing additional functional information on bone marrow vascularization and cellularity.This pictorial review provides an overview of the most important imaging findings in patients with monoclonal gammopathy of undetermined significance, smouldering myeloma and multiple myeloma, by performing a 'total' MRI investigation with implications for the diagnosis, staging and response assessment. Main message • Conventional MRI diagnoses multiple myeloma by assessing the infiltration pattern. • Dynamic contrast-enhanced MRI diagnoses multiple myeloma by assessing vascularization and perfusion. • Diffusion weighted imaging evaluates bone marrow composition and cellularity in multiple myeloma. • Combined morphological and functional MRI provides optimal bone marrow assessment for staging. • Combined morphological and functional MRI is of considerable value in treatment follow-up.
Keywords: Diffusion weighted imaging; Dynamic contrast-enhanced MRI; Magnetic resonance imaging; Multiple myeloma; Response assessment.
Figures














References
-
- Kyle RA, Durie BG, Rajkumar SV, et al. Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management. Leukemia. 2010;24:1121–1127. doi: 10.1038/leu.2010.60. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
