

Idiopathic granulomatous mastitis: a diagnostic dilemma for the breast radiologist
- PMID: 27164916
- PMCID: PMC4956625
- DOI: 10.1007/s13244-016-0497-2
Idiopathic granulomatous mastitis: a diagnostic dilemma for the breast radiologist
Abstract
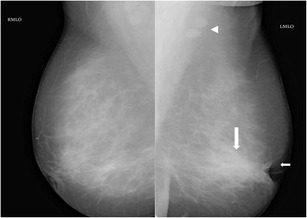
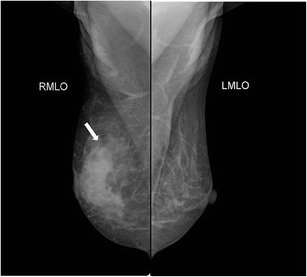
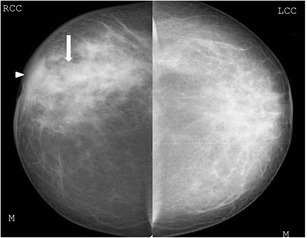
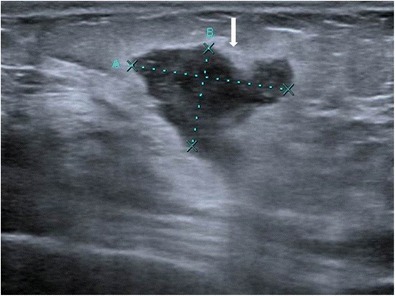
Background: Idiopathic granulomatous mastitis is a chronic inflammatory disease of the breast, which is often difficult to differentiate both clinically and radiologically from infectious aetiologies such as tuberculosis, fungal infections, and also from malignancy, thus posing a diagnostic dilemma. We present a pictorial review of the commonly encountered imaging findings in idiopathic granulomatous mastitis on mammography and ultrasound.
Materials and methods: Mammographic and ultrasound findings of histopathologically proven cases of granulomatous mastitis are discussed.
Conclusion: Idiopathic granulomatous mastitis has varied and non-specific appearances on ultrasound and mammography. Histopathology is essential to establish diagnosis.
Teaching points: • Idiopathic granulomatous mastitis often poses a diagnostic dilemma for the radiologist by mimicking malignancy. • It has varied and non-specific appearances on mammography and ultrasound. • Histopathology is mandatory to establish the diagnosis and decide management.
Keywords: Granulomatous; Histopathology; Mammography; Mastitis; Ultrasound.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
