

Long-term effectiveness of sphenopalatine ganglion stimulation for cluster headache
- PMID: 27165493
- PMCID: PMC5405839
- DOI: 10.1177/0333102416649092
Long-term effectiveness of sphenopalatine ganglion stimulation for cluster headache
Erratum in
-
Corrigendum.Cephalalgia. 2016 Oct;36(11):1098. doi: 10.1177/0333102416669292. Epub 2016 Sep 29. Cephalalgia. 2016. PMID: 27586880 Free PMC article. No abstract available.
Abstract
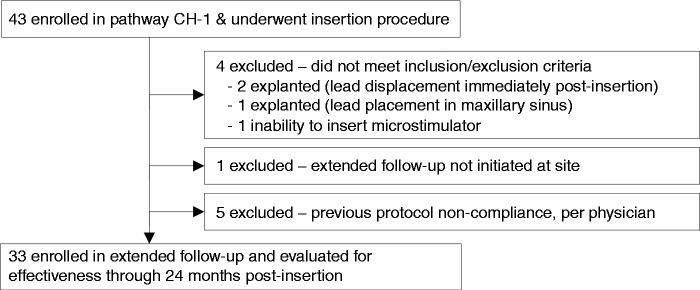
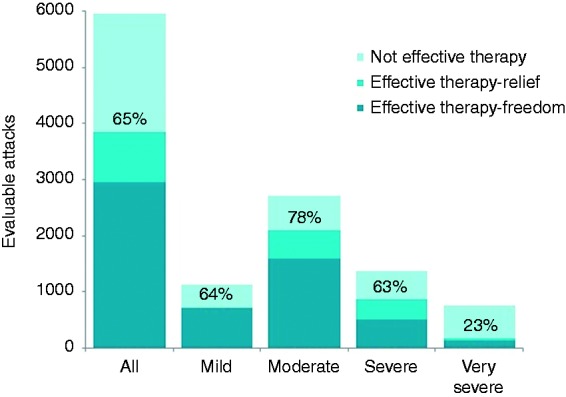
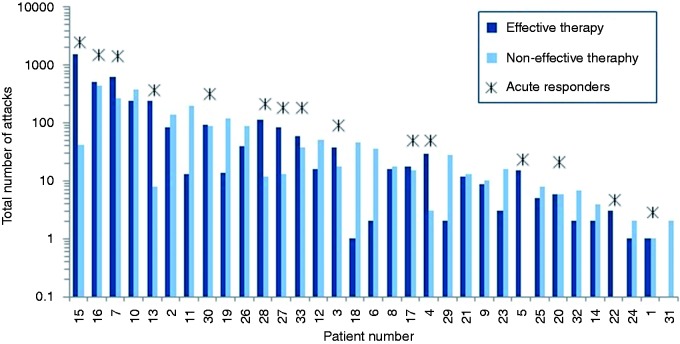
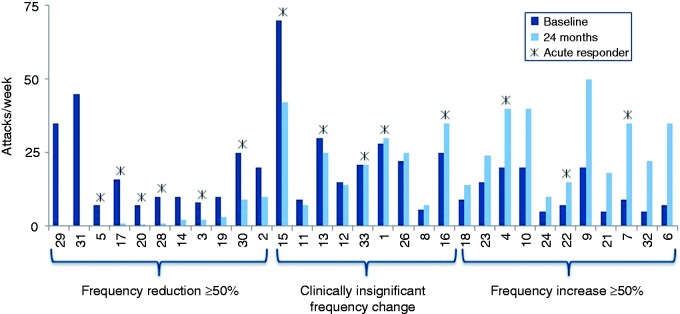
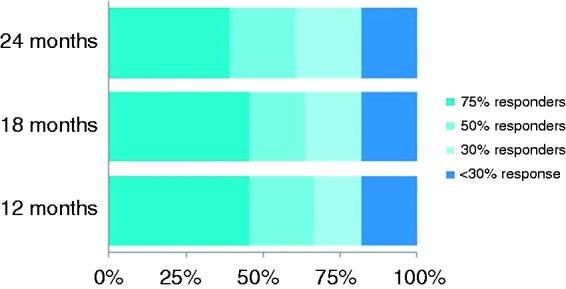
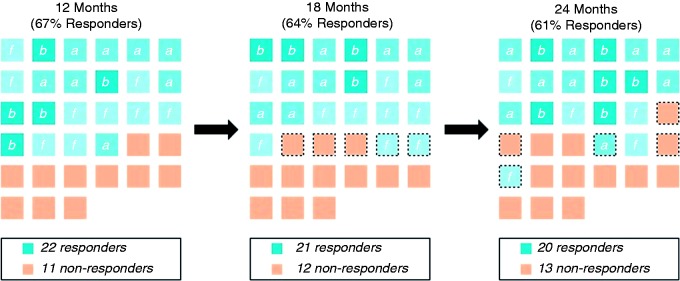
Objectives The sphenopalatine ganglion (SPG) plays a pivotal role in cluster headache (CH) pathophysiology as the major efferent parasympathetic relay. We evaluated the long-term effectiveness of SPG stimulation in medically refractory, chronic CH patients. Methods Thirty-three patients were enrolled in an open-label follow-up study of the original Pathway CH-1 study, and participated through 24 months post-insertion of a microstimulator. Response to therapy was defined as acute effectiveness in ≥ 50% of attacks or a ≥ 50% reduction in attack frequency versus baseline. Results In total, 5956 attacks (180.5 ± 344.8, range 2-1581 per patient) were evaluated. At 24 months, 45% ( n = 15) of patients were acute responders. Among acute responders, a total of 4340 attacks had been treated, and in 78% of these, effective therapy was achieved using only SPG stimulation (relief from moderate or greater pain or freedom from mild pain or greater). A frequency response was observed in 33% ( n = 11) of patients with a mean reduction of attack frequency of 83% versus baseline. In total, 61% (20/33) of all patients were either acute or frequency responders or both. The majority maintained their therapeutic response through the 24-month evaluation. Conclusions In the population of disabled, medically refractory chronic CH patients treated in this study, SPG stimulation is an effective acute therapy in 45% of patients, offering sustained effectiveness over 24 months of observation. In addition, a maintained, clinically relevant reduction of attack frequency was observed in a third of patients. These long-term data provide support for the use of SPG stimulation for disabled patients and should be considered after medical treatments fail, are not tolerated or are inconvenient for the patients.
Keywords: Cluster headache; long-term effectiveness; neuromodulation; neurostimulation; sphenopalatine ganglion.
Figures

References
-
- The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013; 33: 629–808. - PubMed
-
- Jensen RM, Lyngberg A, Jensen RH. Burden of cluster headache. Cephalalgia 2007; 27: 535–541. - PubMed
-
- Jurgens TP, Gaul C, Lindwurm A, et al. Impairment in episodic and chronic cluster headache. Cephalalgia 2011; 31: 671–682. - PubMed
-
- May A, Leone M, Afra J, et al. EFNS guidelines on the treatment of cluster headache and other trigeminal-autonomic cephalalgias. Eur J Neurol 2006; 13: 1066–1077. - PubMed
-
- Leroux E, Valade D, Taifas I, et al. Suboccipital steroid injections for transitional treatment of patients with more than two cluster headache attacks per day: a randomised, double-blind, placebo-controlled trial. Lancet Neurol 2011; 10: 891–897. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
