

Does case management for patients with heart failure based in the community reduce unplanned hospital admissions? A systematic review and meta-analysis
- PMID: 27165648
- PMCID: PMC4874181
- DOI: 10.1136/bmjopen-2015-010933
Does case management for patients with heart failure based in the community reduce unplanned hospital admissions? A systematic review and meta-analysis
Abstract
Objectives: The aim of this systematic review of randomised controlled trials (RCTs) and controlled trials (non-RCTs, NRCTs) is to investigate the effectiveness and related costs of case management (CM) for patients with heart failure (HF) predominantly based in the community in reducing unplanned readmissions and length of stay (LOS).
Setting: CM initiated either while as an inpatient, or on discharge from acute care hospitals, or in the community and then continuing on in the community.
Participants: Adults with a diagnosis of HF and resident in Organisation for Economic Co-operation and Development countries.
Intervention: CM based on nurse coordinated multicomponent care which is applicable to the primary care-based health systems.
Primary and secondary outcomes: Primary outcomes of interest were unplanned (re)admissions, LOS and any related cost data. Secondary outcomes were primary healthcare resources.
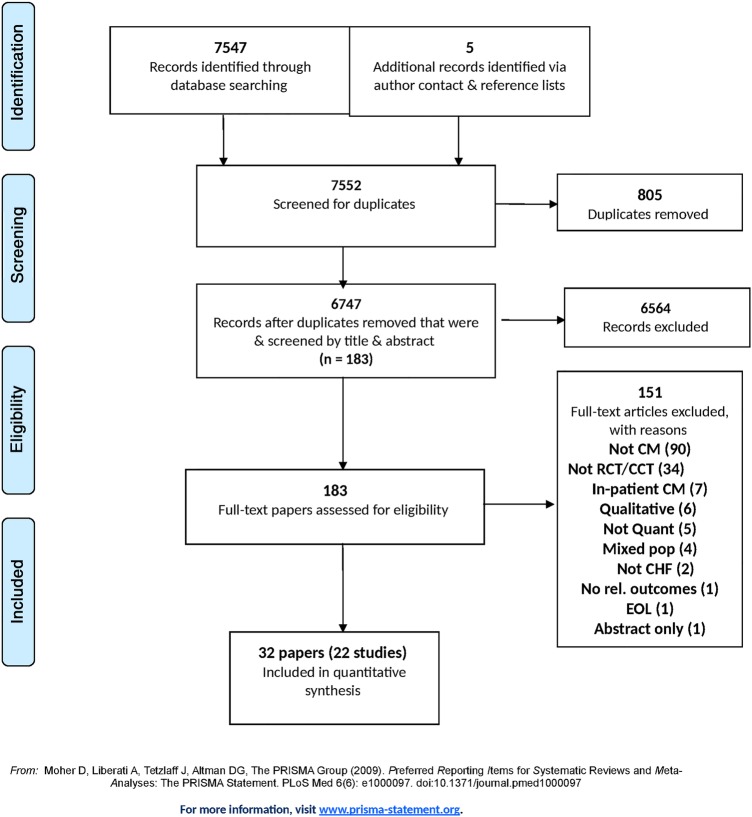
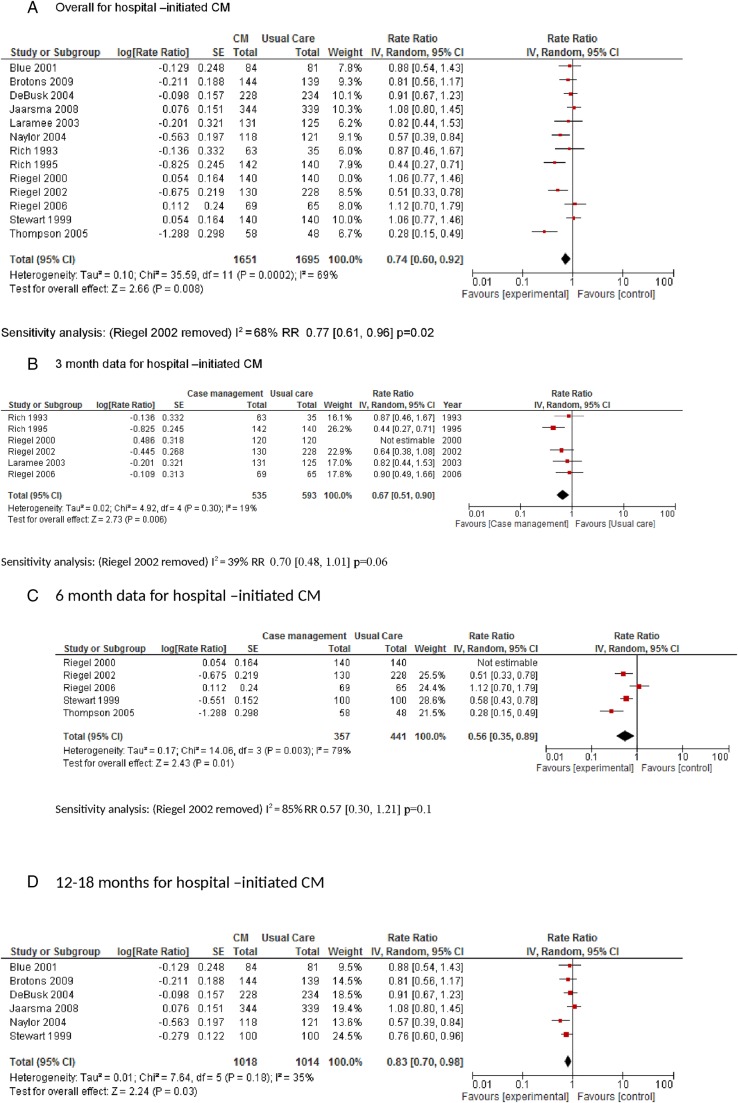
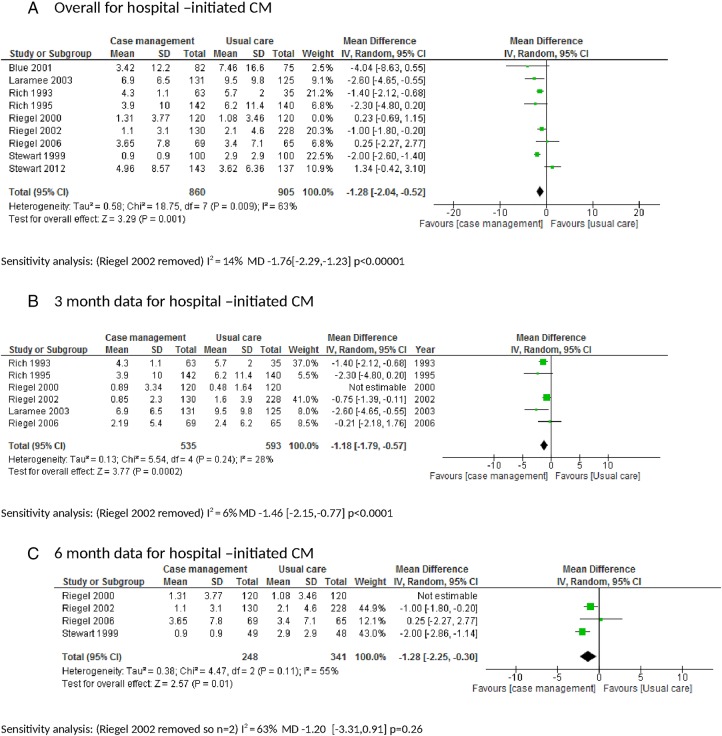
Results: 22 studies were included: 17 RCTs and 5 NRCTs. 17 studies described hospital-initiated CM (n=4794) and 5 described community-initiated CM of HF (n=3832). Hospital-initiated CM reduced readmissions (rate ratio 0.74 (95% CI 0.60 to 0.92), p=0.008) and LOS (mean difference -1.28 days (95% CI -2.04 to -0.52), p=0.001) in favour of CM compared with usual care. 9 trials described cost data of which 6 reported no difference between CM and usual care. There were 4 studies of community-initiated CM versus usual care (2 RCTs and 2 NRCTs) with only the 2 NRCTs showing a reduction in admissions.
Conclusions: Hospital-initiated CM can be successful in reducing unplanned hospital readmissions for HF and length of hospital stay for people with HF. 9 trials described cost data; no clear difference emerged between CM and usual care. There was limited evidence for community-initiated CM which suggested it does not reduce admission.
Keywords: case management; hospital admission; meta-analysis; systematic review.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Cardiovascular disease statistics 2014 British Heart Foundation. https://www.bhf.org.uk/~/media/files/publications/research/bhf_cvd-stati... on the 7/10/2015.
-
- Quality and Outcomes Framework Achievement, prevalence and exceptions data 2012/13. 29 October 2013. http://www.hscic.gov.uk/catalogue/PUB12262/qual-outc-fram-12-13-rep.pdf on the 7/10/2015.
-
- Stewart S, MacIntyre K, Hole DJ et al. More ‘malignant’ than cancer? Five-year survival following a first admission for heart failure. Eur J Heart Fail 2001;3:315–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous